munchkin, that is the goal of the paper. balloon selection will be based upon the circumference of the vein above and below the point of stenosis.munchkin wrote:Dr. S
Thank you for your work with IVUS, what an amazing reduction in vein injury.
Based on the reduction of trauma to the vein using IVUS have you been able to recommend parameters on sizing of balloons based on the corresponding vein size?
Will this information help establish a set of guidelines for treatment protocols?
DrSclafani answers some questions
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
its possible.mo_en wrote:May i add (ask) that muscles of the neck and upper back with reduced flexibility due to venous outflow obstructions put more strain on neck veins and thus worsen the outflow problem itself (?).
we need other clinical specialties to do this work with us!
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Cece wrote:What a great weekend this would be for a case report!
Or is there nothing new under the sun to show us?
(I understand too if time is short and duties long.)
Cece
great case today. Will share tomorrow
S
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Dr. S,drsclafani wrote:its possible.mo_en wrote:May i add (ask) that muscles of the neck and upper back with reduced flexibility due to venous outflow obstructions put more strain on neck veins and thus worsen the outflow problem itself (?).
we need other clinical specialties to do this work with us!
I gather that you have some insight on the muscle issues in the neck and upper back. IMO this a common complaint in MS and other diseases.
Can you give more info, food for thought as this in itself must be part of a cycle effect where it effects posture and then compounds flow issues and nerve conduction issues. Some thing I have personally experienced and hear of in my MS community.
Thanks, Nigel
Re: DrSclafani answers some questions
That is happy news.drsclafani wrote:Cece
great case today. Will share tomorrow
S
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
glad you are a poster child for ccsvi. you are a lucky one. not everyone has such great responses. but it could not happen to a nicer woman.pelopidas wrote:I had a terrible chronic neck pain and occipital headache (in the back of my head) for the past 7-8 years.
MRI showed some mildly prolapsed cervical disk, so i thought i would live with it forever. I was having physiotherapy and i was taking pain killers almost every second day.
Then, 6 months ago (6/10/2011) i had my angioplasty procedure.
One month later i was talking to Dr Sclafani about the great improvements i already had. I mentioned that my neck pain was unexpectedly disappeared. He replied only "Ah, it was the spasm!"
I found what he meant:
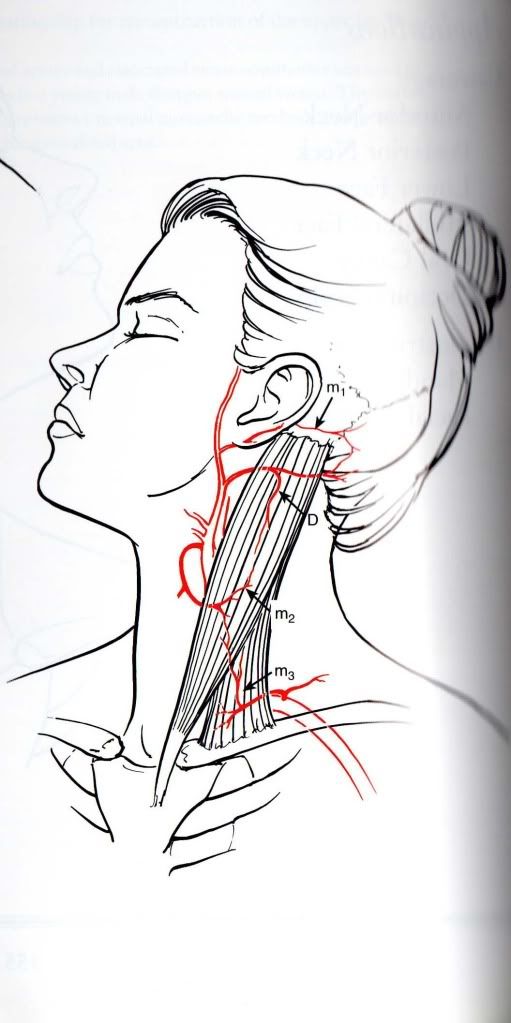
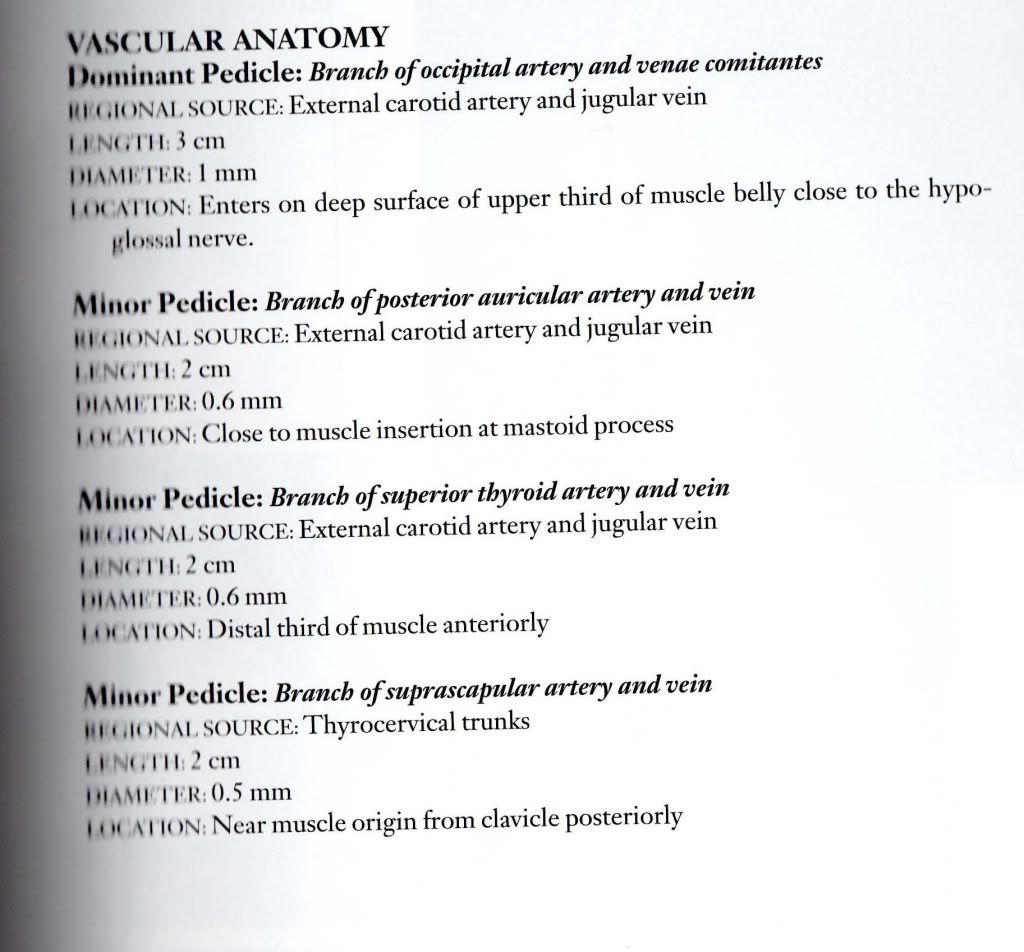
this is the anatomy and the vessels of the sternocleidomastoid muscle (only the arteries here, the veins were of no importance until recently)
almost 90% of this pair of muscles has venous outflow through the jugulars
Maybe the spasm was some symptom of venous congestion of the muscles.
I am relieved of the neck pain and i can turn and flex my head so easily now.
I hope that this will last forever and so will all my other improvements.
Maybe other people have experienced the same thing.
Muscles have veins, too!
Thank you again Dr Sclafani (and this one is a special 6 months post-op thank you)!
-and thank you Cece for the image uploading advice!
a hint on sharing images on TIMS: dont use URL, use
very interesting hypothesis regarding reduction of neck pain.what about this consideration: patients with MS often havfe very large condylar emissary veins that connect to the veins in the posterior neck. Could relieving the resistance in the IJV, reduce flow through the emissary vein and thus reduce venous congestion in the neck muscles?
Sal
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Here you go, Cece. A very interesting case indeed. Not completely resolved yet, but very illustrative of some of the complexity of CCSVI management.Cece wrote:That is happy news.drsclafani wrote:Cece
great case today. Will share tomorrow
S
The patient is a 59 year old Canadian Caucasian female diagnosed initially with relapsing remitting multiple sclerosis in 1971. She was treated by steroids for very infrequent relapses over the first 25-30 years but there was gradual deterioration of function and she appears to have regressed to the secondary progressive form of the disease 6-8 years ago. Her initial symptoms were numbness and fatigue, but she has gradually developed and currently exhibits severe weakness in both lower extremities, spotty numbness in both legs and both arms with varying degrees of loss of light touch and sharp/dull discrimination, with intact positional sense and stereognosis. She uses a scooter primarily because of severe imbalance (Rhomberg's test is grossy abnormal) and to a less degree because of weakness. She has MS hugs predominantly in the extremities, has heat intolerance, and spasms in her legs. She has urinary urgency and frequent nocturia.
In October 2010 she underwent (with another IR) venography and angioplasty. Bilateral internal jugular venoplasty was performed with excellent flow on the right and poor outflow on the left after venoplasty. While unclear, it appears that left jugular stenting was performed because of this poor outflow. Azygography was interpreted as normal.
She had fairly early and increasing improvements in fatigue, numbness and tingling and motor weakness and she greatly improved her activities and her exercising. However imbalance persisted.
In the past two months she has regressed and many of her symptoms are returning and she sought consultation with me.
My examination was pertinent for grossly positive Rhomberg sign, severe weakness in both lower extremities (left worse than right), patchy numbness and insensitivity to light and sharp touch, , inability to walk, and a mottled erythema in both lower extremities.
Venography was performed via a left saphenous approach. I will show representative images and then follow with more detail:
RIGHT INTERNAL JUGULAR VENOGRAM:

LEFT INTERNAL JUGULAR VENOGRAM:

AZYGOUS VENOGRAPHY:

LEFT RENAL VENOGRAPHY:

Any questions?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
That just hurts to see. But you were able to get the catheter through it.drsclafani wrote: LEFT INTERNAL JUGULAR VENOGRAM:
I have not seen many renal venograms yet, so cannot say for sure, but is that nutcracker syndrome?
-
elliberato

- Family Member
- Posts: 82
- Joined: Wed Aug 04, 2010 2:00 pm
- Contact:
Re: DrSclafani answers some questions
can she walk or has she seen any improvements since your procedure?
Re: DrSclafani answers some questions
Can you post the azygous IVUS images, pls?
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
eliberato:elliberato wrote:can she walk or has she seen any improvements since your procedure?
The procedure was concluded and she was discharged yesterday around 1:30 pm. Your expectations are too high.
Let's ask and answer some questions and let this case unfold. The story is just begun.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
what do you think that i got through? What do you see in the jugular view?Cece wrote:That just hurts to see. But you were able to get the catheter through it.drsclafani wrote: LEFT INTERNAL JUGULAR VENOGRAM:
I have not seen many renal venograms yet, so cannot say for sure, but is that nutcracker syndrome?
the nutcracker syndrome requires venographic or CT evidence of obstruction, typically where the renal vein enters the inferior vena cava, collateral flow, symptoms. What do you see? Does the history have any symptoms of nutcracker?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
What do you see on the venogram? I will show the IVUS of everything in good time.bestadmom wrote:Can you post the azygous IVUS images, pls?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
It looks like theres an obstruction at the arc of the azygous, just to the right of where it bulges.
Re: DrSclafani answers some questions
The right internal jugular has a messy valvular area and a curious stenosis above it. Is it the external jugular receiving some dye?
The left internal must have severe intimal hyperplasia because of the stent around its upper side, leaving only a small channel for the catheter. The dye goes all around the other side to the right internal jugular which means that the confluence of sinuses is clear inside the head.
In the azygous view, is there a dye congestion/reverse flow in the lower branches or just an early picture?
The left internal must have severe intimal hyperplasia because of the stent around its upper side, leaving only a small channel for the catheter. The dye goes all around the other side to the right internal jugular which means that the confluence of sinuses is clear inside the head.
In the azygous view, is there a dye congestion/reverse flow in the lower branches or just an early picture?