
That's interesting. The single biggest symptom relief of my wifes CCSVI procedure was eyesight. Back then she had both jugulars and the azygos ballooned, nothing renal was looked at (12/2010). Sadly this has regressed, although it did take a good while to do so.drsclafani wrote:
this presentation and history and outcome make no sense to me. While i have seen vision improved by treating nutcracker, i have never seen improvements related to embolization of gonadal veins. Indeed, i have seen the opposite: that treatment of gonadal vein reflux without treating the nutcracker makes symptoms worsen
DrSclafani answers some questions
Re: DrSclafani answers some questions
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
lets try to illustrate some of the problems of the prior treatments.drsclafani wrote:Thinking about the first three years of CCSVI management, i have noted with alarming frequency some of the errors that were made commonly by proceduralists. Today a very disappointing story illustrated this and points to some explanations for many of the fleeting improvements that many patient experience after angioplasty
The patient was a middle aged Canadian woman with relapsing remitting MS that had progressed into the secondary stage. Her symptoms included chronic debilitating fatigue, temperature intolerance, imbalance, problems with memory and cognition, numbness and tingling and weakness in the extremities and bladder difficulties.
In 2010 she was treated in a European facility. The venogram was interpreted as showing valvular stenosis of the left internal jugular vein at the inferior jugular bulb, and incorrectly diagnosed a normal right internal jugular vein and normal azygous vein. The angiography was poor with very minimal contrast media. However to my eye, valvular stenoses of both the right IJV and the Azygous arch were clearly evident. Angioplasty of the left IJV was performed with a stent that was too small for that vein. Not surprisingly follow up venography was interpreted as showing inadequate angioplasty. Instead of increasing balloon size, stenting was performed. The patient was given a few days of anticoagulation and discharged. some of her symptoms improved, others did not and then some of the improvements regressed.
In 2011 she went to another facility in Europe and imaging was repeated. This second interventionalist detected the right IJV valvular stenosis and treated that successfully. Extensive intimal hyperplasia of the stented left IJV had developed and this has resulted in a narrowing of the lumen in the stent by about 70%. The Left IJV was treated by angioplasty of the stent without additional stenting. Azygous venography again was misinterpreted as normal and again left untreated. Surprisingly, left renal venography was also performed. I saw reflux into the left ovarian vein and was consistent with the renal vein compression syndrome. No intervention was performed.
most would consider this patient to have failed venoplasty. In reality this has just been unsatisfactory treatment. it has take three session to diagnose the critical pathology and some of the lesions still have not been treated. Moreover an unnecessary stent has been ultilized and this will likely lead to a chronic stenosis of the left IJV
hopefully i can address some of these problems tomorrow
2010 First procedure
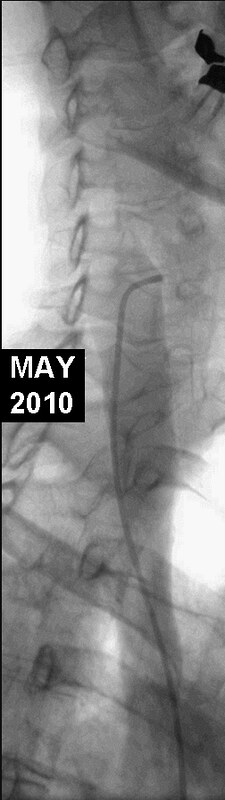
This image began the procedure in 2010. No definite abnormality is seen. HOWEVER, the upper two thirds of the internal jugular vein were not imaged. The catheter is nowhere near the upper portions of the jugular vein. The technique of venography was too slowly inject contrast so that transit time can be assessed. The result is limited contrast media that does not completely opacify the lumen and it does not adequately demonstrate pathology of valves or reveal stenoses. Subtraction technique may have revealed a stenosis but we do not know whether subtraction was actually performed.
Next the left internal jugular vein was imaged:
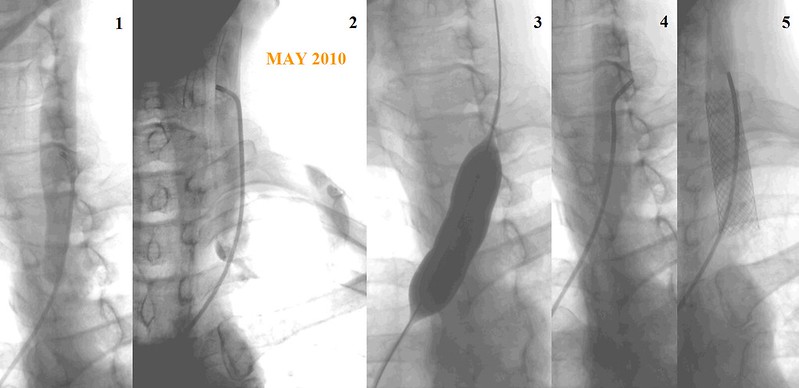
Figure 1 definitely shows a rounded end of the contrast column at the site of a stenosis.
Figure 2 shows added contrast on the left side of the stenosis indicative of contrast under a immobile valve. A slight jet may be seen on the right side of the end of the contrast media.
Figure 3. I think treatment was justified. However, I am not sure sufficient treatment was performed. The balloon is inflated but no waist is seen. A waist is seen when a balloon is stretching the obstruction. In this case the balloon may be too small or of insufficient pressure.
Figure 4. This followup study is just not sufficient to justify stenting. The contrast study is poor. the amount of contrast media is just inadequate to make a definitive diagnosis of stenosis. It might be present but this study is just indefinite. stenosis cannot be ruled out.
Figure 5. A 16mm stent is deployed. It may be considerably larger than the vein.
Azygous venography was performed.
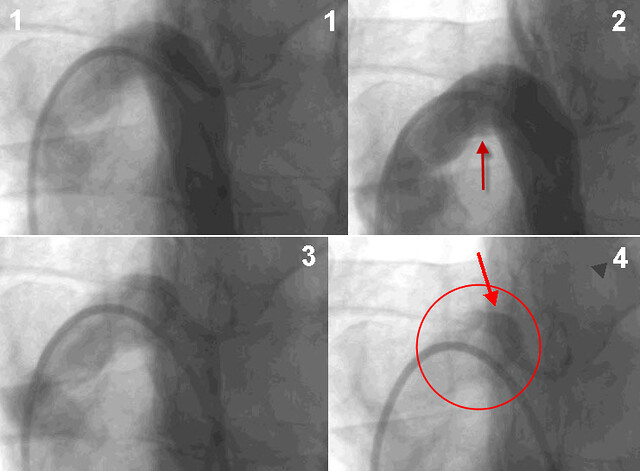
figure 1. looks pretty good. But figure 2. shows reflux into accessory hemiazygous veins. Figure 4 shows contrast trapped underneath the valve leaflets (red circle and red arrow). This is indicative of an immobile valve. I consider this study to be diagnostic. Unfortunately, no treatment was performed.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
How upsetting that the Canadian $6million trial is using IRs who have never done a CCSVI procedure. It is as if it were still 2010. Same errors, same learning curve.
Some of the technique errors in this example were:
* contrast too light to show the vein or the valves adequately
* upper portion of jugular not even imaged so who knows if there is a stenosis there
* undersized ballooning
* contrast too light to see if stenosis resolved
* premature use of stent
* too large of a stent used which can contribute to complications such as narrowing of the vein due to excessive regrowth (intimal hyperplasia)
* use of a stent at all outside of specific indications which were not present
* missed stenosis in azygous went without treatment
Thank you for your time spent preparing images.
Some of the technique errors in this example were:
* contrast too light to show the vein or the valves adequately
* upper portion of jugular not even imaged so who knows if there is a stenosis there
* undersized ballooning
* contrast too light to see if stenosis resolved
* premature use of stent
* too large of a stent used which can contribute to complications such as narrowing of the vein due to excessive regrowth (intimal hyperplasia)
* use of a stent at all outside of specific indications which were not present
* missed stenosis in azygous went without treatment
Thank you for your time spent preparing images.
-
blossom

- Family Elder
- Posts: 1394
- Joined: Thu Dec 03, 2009 3:00 pm
- Location: south western pa.
- Contact:
Re: DrSclafani answers some questions
dear dr. sclafani, what i see from happy poet's post as well as nzer1's, ejc, and pelopidas and now mine is that as much as we all hoped that ccsvi was the answer to these symptoms that for whatever reasons have been named ms--it isn't. as you have said you are not treating ms you are treating venous problems. which for some it helped some symptoms-some it didn't and some are much worse off. and, it seems these veins can not with stand repeated angioplasties and some after the first angioplasty the vein is done for.
so as an expert in your field "which i do believe you are" to even have the possibility that there are factors that could and should be ruled out before angioplasty "which is an invasive procedure"--i would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc.
much as a simple plumber--IF he could have some how seen that the pipe did not have flow because of a dent or possibly complete shut off from an outer element and that stress was not taken off before he runs the roto rotor through--even though the roto rotor may clear things up some what and get some flow going on it would not be lasting or as successful as he hoped for. BUT, we patients are not pipes and replacement parts are not as easy to come by and i would hope that sooner and not later experts as yourself and other experts don't step out of their fields--BUT rather embrace one another's expertee's and for the patients suffering with these so called ms or parkinson's etc. you guys will come up a true cause and effect to eleminate these symptoms---instead of what others have come up with "in theory only" - we'll call it ms throw everybody in a bushel and we can treat them all the same. "NOT WORKED TOO WELL HAS IT" well, it has worked very well for the drug co.'s and that's about it.
you had mentiond about how many people had probably had trauma yet did not have problems. but, you can kinda look at- say there are smokers who puff till they're 100 with no cancer yet a friend of mine never touched any tobacco products nor was exposed to much second hand smoke and he's in his 40's and has throat cancer which at first he was told he had it because he smoked. go figure.
all i know is that there are some really good dr.'s as yourself and in other fields that have taken an interest that has been much needed and it's stirring up the dust. but, there would be more benefit for the patients to be looked at individually and info. and expertee shared and compared.-----not saying it will be easy but it gotta start somewhere. like say happy poet's and the others suggestions.
thank you for your time you spend here at tims.
so as an expert in your field "which i do believe you are" to even have the possibility that there are factors that could and should be ruled out before angioplasty "which is an invasive procedure"--i would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc.
much as a simple plumber--IF he could have some how seen that the pipe did not have flow because of a dent or possibly complete shut off from an outer element and that stress was not taken off before he runs the roto rotor through--even though the roto rotor may clear things up some what and get some flow going on it would not be lasting or as successful as he hoped for. BUT, we patients are not pipes and replacement parts are not as easy to come by and i would hope that sooner and not later experts as yourself and other experts don't step out of their fields--BUT rather embrace one another's expertee's and for the patients suffering with these so called ms or parkinson's etc. you guys will come up a true cause and effect to eleminate these symptoms---instead of what others have come up with "in theory only" - we'll call it ms throw everybody in a bushel and we can treat them all the same. "NOT WORKED TOO WELL HAS IT" well, it has worked very well for the drug co.'s and that's about it.
you had mentiond about how many people had probably had trauma yet did not have problems. but, you can kinda look at- say there are smokers who puff till they're 100 with no cancer yet a friend of mine never touched any tobacco products nor was exposed to much second hand smoke and he's in his 40's and has throat cancer which at first he was told he had it because he smoked. go figure.
all i know is that there are some really good dr.'s as yourself and in other fields that have taken an interest that has been much needed and it's stirring up the dust. but, there would be more benefit for the patients to be looked at individually and info. and expertee shared and compared.-----not saying it will be easy but it gotta start somewhere. like say happy poet's and the others suggestions.
thank you for your time you spend here at tims.
Re: DrSclafani answers some questions
blossom wrote:dear dr. sclafani, what i see from happy poet's post as well as nzer1's, ejc, and pelopidas and now mine is that as much as we all hoped that ccsvi was the answer to these symptoms that for whatever reasons have been named ms--it isn't. as you have said you are not treating ms you are treating venous problems. which for some it helped some symptoms-some it didn't and some are much worse off. and, it seems these veins can not with stand repeated angioplasties and some after the first angioplasty the vein is done for.
so as an expert in your field "which i do believe you are" to even have the possibility that there are factors that could and should be ruled out before angioplasty "which is an invasive procedure"--i would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc.
much as a simple plumber--IF he could have some how seen that the pipe did not have flow because of a dent or possibly complete shut off from an outer element and that stress was not taken off before he runs the roto rotor through--even though the roto rotor may clear things up some what and get some flow going on it would not be lasting or as successful as he hoped for. BUT, we patients are not pipes and replacement parts are not as easy to come by and i would hope that sooner and not later experts as yourself and other experts don't step out of their fields--BUT rather embrace one another's expertee's and for the patients suffering with these so called ms or parkinson's etc. you guys will come up a true cause and effect to eleminate these symptoms---instead of what others have come up with "in theory only" - we'll call it ms throw everybody in a bushel and we can treat them all the same. "NOT WORKED TOO WELL HAS IT" well, it has worked very well for the drug co.'s and that's about it.
you had mentiond about how many people had probably had trauma yet did not have problems. but, you can kinda look at- say there are smokers who puff till they're 100 with no cancer yet a friend of mine never touched any tobacco products nor was exposed to much second hand smoke and he's in his 40's and has throat cancer which at first he was told he had it because he smoked. go figure.
all i know is that there are some really good dr.'s as yourself and in other fields that have taken an interest that has been much needed and it's stirring up the dust. but, there would be more benefit for the patients to be looked at individually and info. and expertee shared and compared.-----not saying it will be easy but it gotta start somewhere. like say happy poet's and the others suggestions.
thank you for your time you spend here at tims.
Thanks Blossom for rounding this up so well. I think the analogies work well and when the plumber has problems with an Electrical switch in the system he calls on the Sparkie for help. When the key pad that runs the system by computer he calls the Nerd.
What I think we are all saying is that Patient Heal Thy Self is in full swing and it shouldn't be this way.
We are pushing the fixers to do their best for us and the difference will occur when the Healers converse and pro-actively combine their skills knowledge and experience to achieve a Goal.
To be honest I think we all see this ability to get everyone together is a Skill you have.
How say you?
Big Day for many Down Under tomorrow ;)
Regards,
Nigel
Last edited by NZer1 on Sun Dec 23, 2012 11:59 pm, edited 1 time in total.
Re: DrSclafani answers some questions
Dr Sclafani, I can only echo what Blossom wrote. And I too would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc. It all seemed so simple 3 years ago, angioplasty was the answer to our problems. With the thousands of patients that have undergone angioplasty, what is clear, is that it does not work for everyone. And for too many of us we are now worse than before this procedure. In an ideal world, doctors in your field could foresee which patients would benefit from angioplasty and which ones would not and avert any worsening of symptoms.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I am trying to show with illustrations is that many patients have undergone less than optimal venoplasty procedures and that these should not be the standard.dania wrote:Dr Sclafani, I can only echo what Blossom wrote. And I too would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc. It all seemed so simple 3 years ago, angioplasty was the answer to our problems. With the thousands of patients that have undergone angioplasty, what is clear, is that it does not work for everyone. And for too many of us we are now worse than before this procedure. In an ideal world, doctors in your field could foresee which patients would benefit from angioplasty and which ones would not and avert any worsening of symptoms.
I am more than willing to take in other theories that I can understand. Please send me peer reviewed references that are published and i will read them and render my own opinion. But I must say that the papers of the University of the Internet do not count. If all I had heard about ccsvi was what I had read on the internet, I would not have become involved. It required the study of countless papers, not abstracts, not internet newsletters, or other opinions. I reviewed some of the abstracts for presentation at the International Society for NeuroVascular Disease and did not see any proposals for presentation on this subject. I am at a loss
Dania
i disagree that multiple angioplasties are not possible. I have no evidence or experience that shows that patients veins do not tolerate more than one angioplasty. I am truly sorry that your experience was so dismal. But it is not the experience that i have had
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
send me some peer reviewed literature and i will try to understand.NZer1 wrote:blossom wrote:dear dr. sclafani, what i see from happy poet's post as well as nzer1's, ejc, and pelopidas and now mine is that as much as we all hoped that ccsvi was the answer to these symptoms that for whatever reasons have been named ms--it isn't. as you have said you are not treating ms you are treating venous problems. which for some it helped some symptoms-some it didn't and some are much worse off. and, it seems these veins can not with stand repeated angioplasties and some after the first angioplasty the vein is done for.
so as an expert in your field "which i do believe you are" to even have the possibility that there are factors that could and should be ruled out before angioplasty "which is an invasive procedure"--i would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc.
much as a simple plumber--IF he could have some how seen that the pipe did not have flow because of a dent or possibly complete shut off from an outer element and that stress was not taken off before he runs the roto rotor through--even though the roto rotor may clear things up some what and get some flow going on it would not be lasting or as successful as he hoped for. BUT, we patients are not pipes and replacement parts are not as easy to come by and i would hope that sooner and not later experts as yourself and other experts don't step out of their fields--BUT rather embrace one another's expertee's and for the patients suffering with these so called ms or parkinson's etc. you guys will come up a true cause and effect to eleminate these symptoms---instead of what others have come up with "in theory only" - we'll call it ms throw everybody in a bushel and we can treat them all the same. "NOT WORKED TOO WELL HAS IT" well, it has worked very well for the drug co.'s and that's about it.
you had mentiond about how many people had probably had trauma yet did not have problems. but, you can kinda look at- say there are smokers who puff till they're 100 with no cancer yet a friend of mine never touched any tobacco products nor was exposed to much second hand smoke and he's in his 40's and has throat cancer which at first he was told he had it because he smoked. go figure.
all i know is that there are some really good dr.'s as yourself and in other fields that have taken an interest that has been much needed and it's stirring up the dust. but, there would be more benefit for the patients to be looked at individually and info. and expertee shared and compared.-----not saying it will be easy but it gotta start somewhere. like say happy poet's and the others suggestions.
thank you for your time you spend here at tims.
Thanks Blossom for rounding this up so well. I think the analogies work well and when the plumber has problems with an Electrical switch in the system he calls on the Sparkie for help. When the key pad that runs the system by computer he calls the Nerd.
What I think we are all saying is that Patient Heal Thy Self is in full swing and it shouldn't be this way.
We are pushing the fixers to do their best for us and the difference will occur when the Healers converse and pro-actively combine their skills knowledge and experience to achieve a Goal.
To be honest I think we all see this ability to get everyone together is a Skill you have.
How say you?
Big Day for many Down Under tomorrow ;)
Regards,
Nigel
Do you understand that for me to be a bridge, I have to see both sides of the sea
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
blossomblossom wrote:dear dr. sclafani, what i see from happy poet's post as well as nzer1's, ejc, and pelopidas and now mine is that as much as we all hoped that ccsvi was the answer to these symptoms that for whatever reasons have been named ms--it isn't. as you have said you are not treating ms you are treating venous problems. which for some it helped some symptoms-some it didn't and some are much worse off. and, it seems these veins can not with stand repeated angioplasties and some after the first angioplasty the vein is done for.
so as an expert in your field "which i do believe you are" to even have the possibility that there are factors that could and should be ruled out before angioplasty "which is an invasive procedure"--i would hope that you and dr.'s in your field would become open to the other research being done and not close the door as what seems to have happened with neuro.'s etc.
much as a simple plumber--IF he could have some how seen that the pipe did not have flow because of a dent or possibly complete shut off from an outer element and that stress was not taken off before he runs the roto rotor through--even though the roto rotor may clear things up some what and get some flow going on it would not be lasting or as successful as he hoped for. BUT, we patients are not pipes and replacement parts are not as easy to come by and i would hope that sooner and not later experts as yourself and other experts don't step out of their fields--BUT rather embrace one another's expertee's and for the patients suffering with these so called ms or parkinson's etc. you guys will come up a true cause and effect to eleminate these symptoms---instead of what others have come up with "in theory only" - we'll call it ms throw everybody in a bushel and we can treat them all the same. "NOT WORKED TOO WELL HAS IT" well, it has worked very well for the drug co.'s and that's about it.
you had mentiond about how many people had probably had trauma yet did not have problems. but, you can kinda look at- say there are smokers who puff till they're 100 with no cancer yet a friend of mine never touched any tobacco products nor was exposed to much second hand smoke and he's in his 40's and has throat cancer which at first he was told he had it because he smoked. go figure.
all i know is that there are some really good dr.'s as yourself and in other fields that have taken an interest that has been much needed and it's stirring up the dust. but, there would be more benefit for the patients to be looked at individually and info. and expertee shared and compared.-----not saying it will be easy but it gotta start somewhere. like say happy poet's and the others suggestions.
thank you for your time you spend here at tims.
I now find this to have a bit of bullying.
What exactly did you read in pelopidas' post that said that venoplasty did not work? I didnt read your conclusion
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
It is the norm that venous dilatations will regress with time. Venoplasty used for dialysis maintenance needs be done as often as every three to six months.EJC wrote:That's interesting. The single biggest symptom relief of my wifes CCSVI procedure was eyesight. Back then she had both jugulars and the azygos ballooned, nothing renal was looked at (12/2010). Sadly this has regressed, although it did take a good while to do so.drsclafani wrote:
this presentation and history and outcome make no sense to me. While i have seen vision improved by treating nutcracker, i have never seen improvements related to embolization of gonadal veins. Indeed, i have seen the opposite: that treatment of gonadal vein reflux without treating the nutcracker makes symptoms worsen
The resistance to support is the real problem of venoplasty and hopefully there will be some movement on publications beyond safety studies although these are quite expensive to perform.
I always look at regressions and restorations by additional angioplasties to be circumstantial evidence of a cause / effect relationship.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com

Re: DrSclafani answers some questions
Dr. Sclafani, I did not know about your regret until now--thank you for explaining. Please understand that I push for collaboration between doctors for my daughter who has started to exhibit neurological symptoms and for all the other youth who already have been or will be diagnosed with this monster.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
yes, happypoetHappyPoet wrote:Dr. Sclafani, I did not know about your regret until now--thank you for explaining. Please understand that I push for collaboration between doctors for my daughter who has started to exhibit neurological symptoms and for all the other youth who already have been or will be diagnosed with this monster.
to have caused in my wife even transient ccsvi symptoms by untempered enthusiasm for a new treatment has been sobering. i remain hopefully but cautious and skeptical about ccsvi treatments. I am against supporting anything that i cannot accept or understand based upon peer reviewed literature, basic accepted truths and my own experience and logic
if i do, please stop me
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
So far there is very little on peer reviewed literature. CCSVI is so very new.
http://www.fonar.com/pdf/PCP41_damadian.pdf.
http://www.fonar.com/pdf/PCP41_damadian.pdf.
Re: DrSclafani answers some questions
Nigel, you made very good points. Thanks for participating in the discussion 2X.
EJC, I understand what you're saying. Hopefully one day medical training in the US will become more inclusive and multidisciplinary.
blossom, you have the biggest heart I know. You're always crusading for the individual patient, and you're also always advocating for cooperation between doctors. Thank you! If you're a bully, then I'm a bully, too, and I'll be at your side in these quests for as long as I can.
Dr. Sclafani, thank you for reaching out to Nigel and dania. We understand that you want to be the best CCSVI IR you can be and that IR is where your interests lie, but we selfishly ask that you go beyond this amazing commitment to learn about and become familiar with other specialties. Thank you for walking this bridge to see the other side of the sea.
Edits in blue.
EJC, I understand what you're saying. Hopefully one day medical training in the US will become more inclusive and multidisciplinary.
blossom, you have the biggest heart I know. You're always crusading for the individual patient, and you're also always advocating for cooperation between doctors. Thank you! If you're a bully, then I'm a bully, too, and I'll be at your side in these quests for as long as I can.
Dr. Sclafani, thank you for reaching out to Nigel and dania. We understand that you want to be the best CCSVI IR you can be and that IR is where your interests lie, but we selfishly ask that you go beyond this amazing commitment to learn about and become familiar with other specialties. Thank you for walking this bridge to see the other side of the sea.
Edits in blue.
Last edited by HappyPoet on Mon Dec 24, 2012 7:53 pm, edited 2 times in total.
Re: DrSclafani answers some questions
Thanks Dr,
it is a good sobering reminder for me to hear your words.
Its too easy to live in hope and then move to the next branch of hope without learning the finer points of a process of fact finding, technique refining and longevity of outcomes.
Thank You everyone and may your God go with you.
Compliments of the season,
Nigel
it is a good sobering reminder for me to hear your words.
Its too easy to live in hope and then move to the next branch of hope without learning the finer points of a process of fact finding, technique refining and longevity of outcomes.
Thank You everyone and may your God go with you.
Compliments of the season,
Nigel