notadoc wrote:http://www.erinelster.com/files/jvsr%20 ... d%2081.pdf
I was one of the subjects in this study by Dr. Elster. I do not agree that my problems should be attributed to the disagreement I had with that horse many years ago, but I do strongly support the hypothesis that the misaligned C1/C2 was impinging on the jugular vein and contributing to the MS symptoms. Fortunately, the stent that Dr. Sclafani placed in that jugular seems to have resolved the problem so I no longer need the upper cervical treatments. That is even more fortunate because Dr. Elster has sold her practice and moved on, plus she would no longer treat me with the stent in place. I hope you will comment on the paper, Dr. S. It has been eleven months since you treated me and everything is great. Great thanks for choosing this route.
Thanks for the followup. And congratulations on successful durable treatment.
Let's review this case. notadoc is a man with relapsing remitting MS for about 12 years, first symptoms being vertigo and ON. Symptoms at presentation included migraines, life style limting fatigue, difficulties with concentration, vertigo, imbalance, tinnitus, numbness and neuopathy on both fee, fingrs and lower legs, temperature intolerance, weakness in legs and neck with spasticity, urinary dysfunction.
He received treatment on October 2010 at another institution with positive results that gradually regressed after six months of benefits. the next six months.
I treated notodoc in January 27, 2012. Let me show the images of the procedure.
right IJV
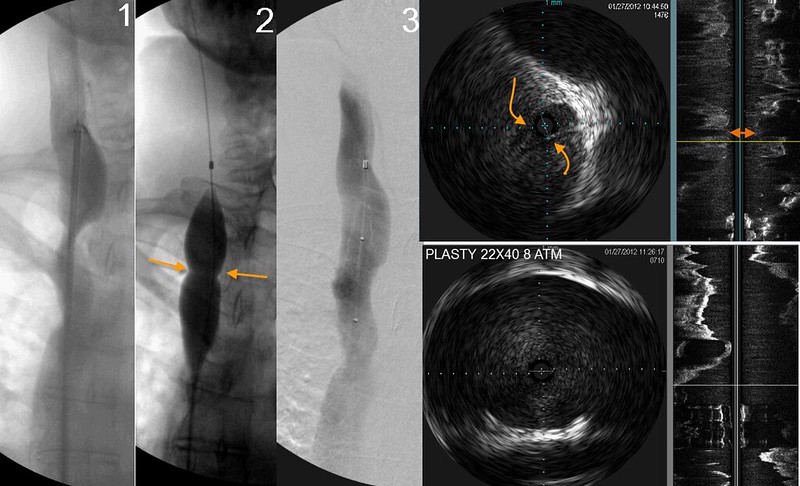
There was high grade stenosis of the right IJV at the confluens. IVUS shows that this is caused by immobile valves and it was treated with a large balloon angioplasty with about 22 atmospheres of pressure. as you can see by ivus and by venography, treatment was successful with a wide open jugular vein.
Left IJV
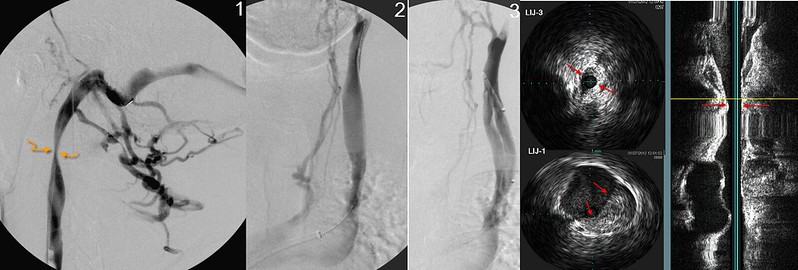
image #1 shows tremendous reflux through numerous emissary veins that drain into the posterior cervical vein. A high grade stenosis at the second cervical vertebra narrowed the vein to less than 2 mm diameter. Flexion/extension, and rotation imaging with IVUS did not show any improvement in luminal area.
image #2 showed those cervical collaterals draining slowly and also showed reflux in pharyngeal veins. A typical valvulare stenosis was seen in the lower J1 segment on both ivus and catheter venography. . I was quite surprised that the apparently large diameter of he middle of the jugular vein actually was an early division into a facial vein and the internal jugular vein. This is important if you do not perform ivus because one could easilyil oversize the balloon based on the apperently large IJV on image #2
Without performing a catheterization of the dural sinus ()image 1), the interventionalist would have missed this upper jugular lesion.
Left IJV treatments
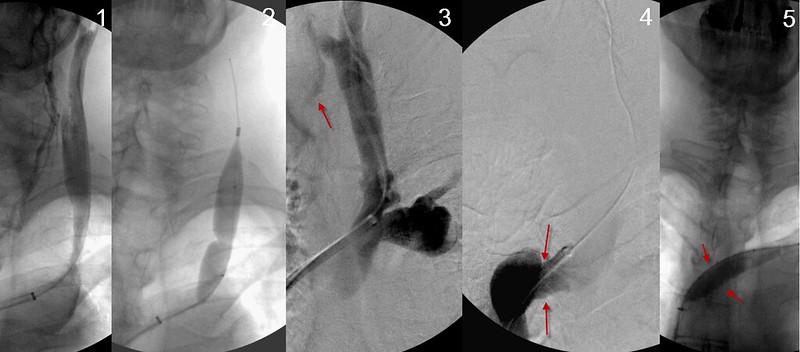
Angioplasty of the J1 segment was pretty good (see image 3). However in the same image one sees collaterals refluxing in image 3 (red arrow). Also look at the dilated subclavian vein to the right of the IJV on image 3, suggesting that there was obstruction in the brachiocephalic vein. Image 4 shows a narrowing in the brachiocephalic vein. We treated that with angioplasty too.
Left J3 treatment
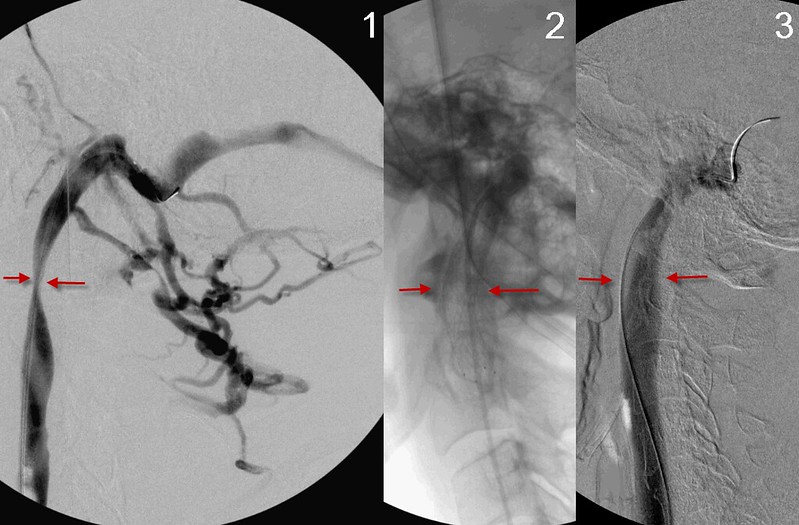
here the focus is on the J3 segment stenosis. It is not located at the skull base, but more inferiorly. I didnt recognize any subluxations on my images. This stenosis is usually caused by a compression and treatment is usually not successful. I haven't put many stents in but I have treated several patients who have had problems with stents placed by others. Problems include migration, kinking, fracture, intimal hyperplasia. I havent seen a thrombosis yet. The details are a bit murky now but i think i treated by stenting because the usual angioplasty of the valves did not result in better flow. After stent placement (see image 3) there is no reflux in the emissary veins and the stenosis is no longer present.
azygos treated too.

Venography did not see a problem but ivus revealed a thickened valvular stenosis in the azygous arch



