DrSclafani answers some questions
Re: DrSclafani answers some questions
I notice too that in the image on the left the patient is not wearing a nose oxygen mask, but in the image on the right, the patient is. Any rationale for when to have a patient wear the little nose mask and when not? I have personal experience with it, for one of my two procedures.

Re: DrSclafani answers some questions
While their similarity extends to their R-IJV and Azygos vein venogram presentations, the similarity ends there; their L-IJVs are very dissimilar. Perhaps the difference in their clinical symptoms is partly due to the severe double stenoses shown on the right--the blood could easily get trapped between the two stenoses and stagnate, becoming sluggish.drsclafani wrote:
I was struck by the similarity of the venographic appearances and the dissimilar clinical presentations.
My study showed that the azygous and right internal jugular vein angioplasties were well maintained with no stenoses, or valvular immobility.
This is a comparison of each patients's left internal jugular veins:

Another difference is their collateral veins (top of images). More blood in the left image, which has one stenosis, finds a route down via a large collateral than does the blood in the right image in which there are very faint collateral veins which means little blood made its way down that route. The blood on the right image must have used other routes not shown on this particular venogram. Perhaps the blood used the vertebral veins (via the sinuses and/or other collateral veins).
But having said all that, I'm not sure the large vein on the top of the left image is a collateral--could that large vein be part of the Left Sigmoid Sinus?
Re: DrSclafani answers some questions
HappyPoet, you are thinking that the one on the right is the son and the one on the left is the mom, because the CCSVI on the right looks worse?
I thought to look for which one looks as if it's benefitted from two prior angioplasties, then thought I could just as well be looking for which one was damaged by two prior angioplasties. The one on the right has a jagged odd look to it down at the bottom.
I thought to look for which one looks as if it's benefitted from two prior angioplasties, then thought I could just as well be looking for which one was damaged by two prior angioplasties. The one on the right has a jagged odd look to it down at the bottom.
Re: DrSclafani answers some questions
Cece, thinking of damage is insightful, and that jagged area is curious. I'm starting to doubt that the large collateral vein of the left image is the L-SS because of the shadowed area under the very dark dye.
The mother and son having 2/3 of the major drainage routes from their CNS being patent is terrific for them. We know DrS will give their L-IJVs the best chance possible, so mother and son are some of the luckier patients, CCSVI-wise. Hopefully, symptom-wise, mother and son will experience longer-lasting or permanent improvements as well as more improvements.
I'm not sure which venogram is of which patient, so I'm really looking forward to the next pieces of information that DrS will be giving us. I'd like to see a venogram with contrast dye shown in their dural sinuses; it will be interesting to see what veins, collateral or otherwise, fill with refluxing dye from their stenosed L-IJVs.
With these two venographic and symptomatic presentations, if I was either patient, I would be grateful to have my dural sinuses investigated. This is the third case in which I'm finding myself questioning my thoughts on imaging of the sinuses. I now believe this investigation is important for patients, just as important as having renal and iliac veins investigaed.
The mother and son having 2/3 of the major drainage routes from their CNS being patent is terrific for them. We know DrS will give their L-IJVs the best chance possible, so mother and son are some of the luckier patients, CCSVI-wise. Hopefully, symptom-wise, mother and son will experience longer-lasting or permanent improvements as well as more improvements.
I'm not sure which venogram is of which patient, so I'm really looking forward to the next pieces of information that DrS will be giving us. I'd like to see a venogram with contrast dye shown in their dural sinuses; it will be interesting to see what veins, collateral or otherwise, fill with refluxing dye from their stenosed L-IJVs.
With these two venographic and symptomatic presentations, if I was either patient, I would be grateful to have my dural sinuses investigated. This is the third case in which I'm finding myself questioning my thoughts on imaging of the sinuses. I now believe this investigation is important for patients, just as important as having renal and iliac veins investigaed.
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
all patients who are getting intravenous sedation or analgesia are supposed to have continuous oxygenCece wrote:I notice too that in the image on the left the patient is not wearing a nose oxygen mask, but in the image on the right, the patient is. Any rationale for when to have a patient wear the little nose mask and when not? I have personal experience with it, for one of my two procedures.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I pushed the envelope for the son, poor guy really needed all the chance possible.Started with five millimeter angioplasty and worked up to a ten mm. Working high and low. the low was the easy stuff. But i suspect that angioplasty is not going to make that much difference.HappyPoet wrote:Cece, thinking of damage is insightful, and that jagged area is curious. I'm starting to doubt that the large collateral vein of the left image is the L-SS because of the shadowed area under the very dark dye.
The mother and son having 2/3 of the major drainage routes from their CNS being patent is terrific for them. We know DrS will give their L-IJVs the best chance possible, so mother and son are some of the luckier patients, CCSVI-wise. Hopefully, symptom-wise, mother and son will experience longer-lasting or permanent improvements as well as more improvements.
I'm not sure which venogram is of which patient, so I'm really looking forward to the next pieces of information that DrS will be giving us. I'd like to see a venogram with contrast dye shown in their dural sinuses; it will be interesting to see what veins, collateral or otherwise, fill with refluxing dye from their stenosed L-IJVs.
With these two venographic and symptomatic presentations, if I was either patient, I would be grateful to have my dural sinuses investigated. This is the third case in which I'm finding myself questioning my thoughts on imaging of the sinuses. I now believe this investigation is important for patients, just as important as having renal and iliac veins investigaed.
In mom, I chose not to push the envelope because she is more function. I think that many hypoplasias end up thrombosing if you work too hard on them.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I think that hypoplasias are really problematic. I think that a maturation procedure might have value but would only be possible in someone who lived locallyCece wrote:As a mom, this is the worst fear.drsclafani wrote:Her 34 year old son was diagnosed with multiple sclerosis at age 31. His course has been unrelenting. Severe cerebellar intention tremors have been incapacitating. Weakness, choking, and no response to medications.
You can see the contrast refluxing at the top of the jugular into collateral veins in both images.This is a comparison of each patients's left internal jugular veins:
The image on the left looks like it has a narrowing near the area of the valves.
The image on the right shows a more complicated flow situation, with apparent stenoses both lower down and up at J3.
Was the prior angioplasty at the area of the valves? Was this J3 stenosis observed and/or treated during the prior treatments? Had IVUS ever been used on these patients? Or the renal or iliac veins checked? I like stories with happy endings....
Did you find a possible explanation as to why patients with similar venograms would have such dissimilar courses?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
pelopidas wrote:"Did you find a possible explanation as to why patients with similar venograms would have such dissimilar courses?"
also, why patients with (as far as we know) dissimilar venograms would have similar courses?
i'm looking forward to the rest of the story of this family case
many rivers that look quite differently have flooded.
i do not see a anatomical correlation between ccsvi and ms
i am not surprised , just touched by the oddness of fate when it comes to MS
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com

Re: DrSclafani answers some questions
Did the son, on the right, have such bad intention tremors that he had to be put totally out with anesthesia, so that he would not shake during the procedure? Some tremors can be so bad the patient can't lay still for even a second. He had to have the oxygen then.
Did he have two very bad stenosis problems that had elastic recoil or the lumina sticking together?
So during his prior procedures he was not helped, no improvements? Were his other two procedures with post-medication? JMO
Did he have two very bad stenosis problems that had elastic recoil or the lumina sticking together?
So during his prior procedures he was not helped, no improvements? Were his other two procedures with post-medication? JMO
Where there is a will, there is a way. "HOPE"
CCSVI Procedure December 2010
CCSVI Procedure December 2010
Re: DrSclafani answers some questions
drsclafani wrote:
many rivers that look quite differently have flooded.
i do not see a anatomical correlation between ccsvi and ms
i am not surprised , just touched by the oddness of fate when it comes to MS
this wise answer seems like a haiku poem!
getafix
-
ErikaSlovakia
- Family Elder
- Posts: 1125
- Joined: Wed Jul 29, 2009 2:00 pm
- Location: Slovakia, Europe
- Contact:
Re: DrSclafani answers some questions
Dear Dr. Sclafani!
It is not my case but one patient has asked me for help.
A woman got 4 stents into her jugulars. One of the stent migrated into her heart.
Either they have noticed couple of months later or it was soon after the intervention. IR tried to "pull" it out but the stent is growed to the ventricle (of her heart).
She is scared of course and does not feel very well. She gets extrasystols and feels pressure on her chest.
She does not know what to expect.
Do you have an idea?
Erika
It is not my case but one patient has asked me for help.
A woman got 4 stents into her jugulars. One of the stent migrated into her heart.
Either they have noticed couple of months later or it was soon after the intervention. IR tried to "pull" it out but the stent is growed to the ventricle (of her heart).
She is scared of course and does not feel very well. She gets extrasystols and feels pressure on her chest.
She does not know what to expect.
Do you have an idea?
Erika
Aug. 7, 09 Doppler Ultras. in Poland, left Jugul. valve problem, RRMS since 1996, now SPMS,
- Nov.3,09: one stent in the left jug. vein in Katowice, Poland, LDN, never on DMDs
- Jan. 19, 11: control venography in Katowice - negative but I feel worse
- Nov.3,09: one stent in the left jug. vein in Katowice, Poland, LDN, never on DMDs
- Jan. 19, 11: control venography in Katowice - negative but I feel worse
Re: DrSclafani answers some questions
A stent in her heart? That is awful, Erika.
So if a mom and son have hypoplastic left jugulars, there would seem to be a genetic cause for the hypoplasias.
It is good that the other veins remained patent. It rather demonstrates the importance of having two fully functional jugulars, if having hypoplasia on one side meant no lasting improvements.
This case also touches on the question of patient selection, as I understand it, if you approached the mom's hypoplasia differently than the son's.
I didn't even recognise these as hypoplasias.drsclafani wrote:I pushed the envelope for the son, poor guy really needed all the chance possible.Started with five millimeter angioplasty and worked up to a ten mm. Working high and low. the low was the easy stuff. But i suspect that angioplasty is not going to make that much difference.
In mom, I chose not to push the envelope because she is more function. I think that many hypoplasias end up thrombosing if you work too hard on them.
So if a mom and son have hypoplastic left jugulars, there would seem to be a genetic cause for the hypoplasias.
It is good that the other veins remained patent. It rather demonstrates the importance of having two fully functional jugulars, if having hypoplasia on one side meant no lasting improvements.
This case also touches on the question of patient selection, as I understand it, if you approached the mom's hypoplasia differently than the son's.
Re: DrSclafani answers some questions
So very sorry about the hypoplasia in both mother and son--you've given them their best opportunity for symptom relief which must be a measure of comfort for them to know they've done everything they could do for their CCSVI. Now we wait and hope their L-IJVs can stay patent like their other veins have been able to do.drsclafani wrote:I pushed the envelope for the son, poor guy really needed all the chance possible.Started with five millimeter angioplasty and worked up to a ten mm. Working high and low. the low was the easy stuff. But i suspect that angioplasty is not going to make that much difference.
In mom, I chose not to push the envelope because she is more function. I think that many hypoplasias end up thrombosing if you work too hard on them.
Did all the blood go down the son's L-IJV after your angioplasty to 10mm, or were collaterals still being used? By what route(s) did the blood take before the angioplasty?
Re: DrSclafani answers some questions
http://www.thisisms.com/forum/chronic-c ... ml#p172379
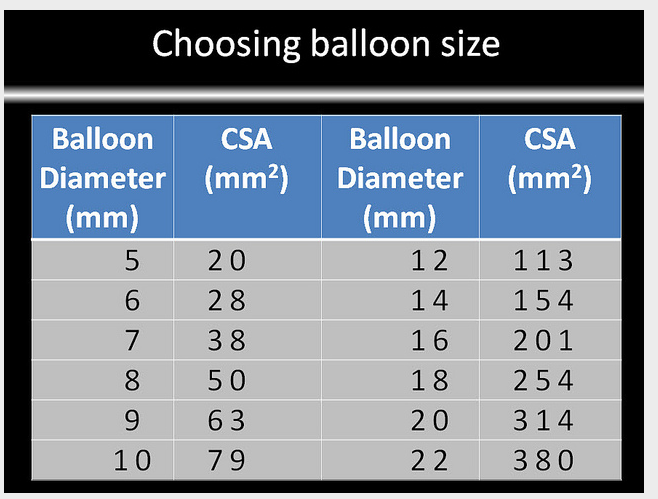
Here is a chart from a previous discussion on balloon sizing.
Previously hypoplasia has been defined as being between 2 - 4 mm in diameter. If we take it as 4 mm, the CSA is only 13 mm2 (CSA = pi*r*r = 3.14*2*2).
13 mm2 is too small to even make it onto this chart. But you normally upsize one level, so if 13 mm2 would have been on the chart across from a 4 balloon, then a 5 balloon should be safe. A 10 balloon means going for broke. A 13 mm2 vein is not much to lose on its own, although what is also lost if it clots down is the potential for future treatments of that vein, should an effective treatment for hypoplasia be found. I do not envy such hard choices.
Maturation remains an interesting concept. Not only would the patient need to be local, but the funding would have to be there for multiple procedures. One difference between arteriovenous fistula maturation and hypoplastic jugular maturation is that the AVF is a high flow environment because of the mixing with an artery and the hypoplastic jugular is a low flow environment. A way to increase the flow through the jugulars is if the patient remains supine, so that the flow goes through the jugulars. It still would not be the high flow environment of the artery, but it would not be as low flow as it gets when a patient is upright. So perhaps the treatment of hypoplasia could be two months filled with procedures, bedrest, procedures, bedrest. If it works, it's worth it.
HappyPoet, you mention that the other veins were able to stay patent. That could mean that the son's veins are resilient, in general, which would be good for this vein's chances.
Here is a chart from a previous discussion on balloon sizing.
Previously hypoplasia has been defined as being between 2 - 4 mm in diameter. If we take it as 4 mm, the CSA is only 13 mm2 (CSA = pi*r*r = 3.14*2*2).
13 mm2 is too small to even make it onto this chart. But you normally upsize one level, so if 13 mm2 would have been on the chart across from a 4 balloon, then a 5 balloon should be safe. A 10 balloon means going for broke. A 13 mm2 vein is not much to lose on its own, although what is also lost if it clots down is the potential for future treatments of that vein, should an effective treatment for hypoplasia be found. I do not envy such hard choices.
Maturation remains an interesting concept. Not only would the patient need to be local, but the funding would have to be there for multiple procedures. One difference between arteriovenous fistula maturation and hypoplastic jugular maturation is that the AVF is a high flow environment because of the mixing with an artery and the hypoplastic jugular is a low flow environment. A way to increase the flow through the jugulars is if the patient remains supine, so that the flow goes through the jugulars. It still would not be the high flow environment of the artery, but it would not be as low flow as it gets when a patient is upright. So perhaps the treatment of hypoplasia could be two months filled with procedures, bedrest, procedures, bedrest. If it works, it's worth it.
HappyPoet, you mention that the other veins were able to stay patent. That could mean that the son's veins are resilient, in general, which would be good for this vein's chances.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
ALL my patients get supplemental oxygen.CD wrote:Did the son, on the right, have such bad intention tremors that he had to be put totally out with anesthesia, so that he would not shake during the procedure? Some tremors can be so bad the patient can't lay still for even a second. He had to have the oxygen then.
Did he have two very bad stenosis problems that had elastic recoil or the lumina sticking together?
So during his prior procedures he was not helped, no improvements? Were his other two procedures with post-medication? JMO
I try to avoid general anesthesia at all costs and in this case i was able to get the job done. It seemed that when i held the hand of the young man during the procedure, his tremors calmed down but he never stopped for more than a minute.
One of the overlooked values of IVUS is its real time nature that allows capture of image data during movement. So I was able to work even when the pictures of the venograms were a bit blurry.
it was not clear whether the prior procedure actually attempted to open the hypoplasia. Given the short lived results, i would suspect elastic recoil of the other treatments.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
- Similar Topics
- Replies
- Views
- Last post