These images have gone the way of your profile picture! Flickr, so fickle....drsclafani wrote:
These images show an IVUS (center) to assure myself of a good apposition between stent and vein wall and nice IVUS (right) and venographic (left) images showing restoration of flow and diameter.
DrSclafani answers some questions
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions

-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: Dural sinus are safe with DrS
Indeed, Disney World is full of characters, but there is only one character in the Brooklyn procedure room.drsclafani wrote:Lest the CCSVI world now spread a story that DrSclafani uses the Liberation Procedure as a recreational tool, let me end the rumor that the procedure room in Brooklyn, New York is my personal Disneyworld. I love m y work, but it ain't a game.
Plus, at Disney World, lots of food. In Brooklyn, no food until you make it to the turkey sandwich in the recovery room.
Also, at Disney World, the magic is pretend. Not so in the Brooklyn procedure room.
-
PointsNorth
- Family Elder
- Posts: 683
- Joined: Mon Sep 04, 2006 2:00 pm
- Location: LeftCoast Canada
- Contact:
Re: DrSclafani answers some questions
I thought that the turkey sandwich was pretty good. Altho it was 6pm and I hadn't eaten all day!
Albany 2010. Brooklyn 2011
Hayes inspired Calcitriol+D3 2013-2014
Coimbra Protocol 2014-16
DrG B12 Transdermal Spray 2014-16
Progesterone 2015-16
Low-Dose Immunotherapy 2015-16
My Current Regimen http://www.thisisms.com/forum/regimens-f22/topic25634.html
Hayes inspired Calcitriol+D3 2013-2014
Coimbra Protocol 2014-16
DrG B12 Transdermal Spray 2014-16
Progesterone 2015-16
Low-Dose Immunotherapy 2015-16
My Current Regimen http://www.thisisms.com/forum/regimens-f22/topic25634.html
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Had there been no collateral there, thrombosis would have continued to propogate toward the headCece wrote:drsclafani wrote:
these are images of the two venograms performed in January. The initial study is on the left three panels and shows an angioplasty of a lesion that is not well seen. A week later there is extensive thrombus in the LIJV.
These are very interesting images. There is a visible collateral in the fourth panel. It definitely looks like the blood flow had worsened from the patient's initial baseline. .

Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
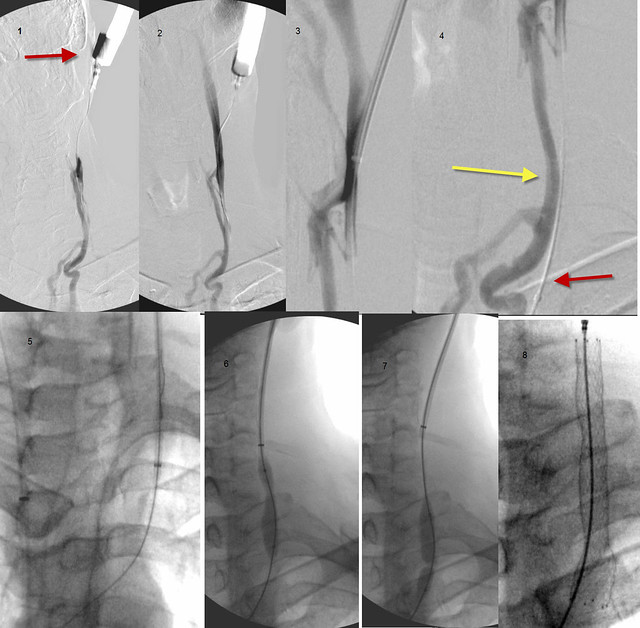
It's interesting that it didn't go into the verts but into the anterior jugular instead.drsclafani wrote:When he consulted me, i learned of the thrombosis so I was preparing to address this issue. A surface ultrasound confirmed the thrombosis. I began a complete diagnostic venogram but very quickly abandoned attempts to catheterize this vein from the femoral side of the catheterizationand went on to direct puncture of the high portion of the IJV via ultrasound guidance.
in window 1 you can see the red arrow pointing to the neck catheterization.
in window 4 most of the contrast material is opacifying the anterior jugular vein (yellow arrow) . You can see how it parallels the IJV (red arrow)
What a difference too between this not-there jugular and the one in the images from January.
Glad to hear it worked.Bridging the thrombosis with a guidewire is the most important and often the most difficult component of this procedure. I used a guidewire first but it just kept getting hung up on this organized thrombus. Next i used a stiffer wire with a J on the tip to atraumatically push the wire through the clot. In this case this technique worked.
I had no idea back in the early days that we would see people lose their jugulars after an attempt to fix their jugulars. It's awful.
So first the guidewire, then the stiffer wire with a 'J' tip, then the stiffer-yet back end of a wire, then a cutting needle if lined up straight (risky), then potentially intravascular RF (risky).
If it didnt work, then I would use the stiffer back end of a wire to push through the clot. If that failed, i would use a cutting needle IF i could assure myself that I was properly lining up the vein on both sides. This is often very challenging because there are adjacent structures such as lung, arteries, sometimes bowels (not in this situation) and other structures that might be injured if the alignment of the needle and the target was not perfect.
Another newer technique is radiofrequency delivery of heat energy to burn through the organized clot. However risks of perforation occur with this technique as well.
How did you predilate the wire track? I am not sure what that means.Thankfully, i was able to get the wire into the more central vein. and then i predilated the wire track.
Next I used a snare to grab a wire from the femoral side and pull it through the thrombosis.
So you had a wire from the upper jugular rendez-vous access point that made it through to the other side.
You also had a wire that had come up from the femoral access point in the groin.
I am not sure which side the snare came from or how it got where it needed to be?
The wire that had come up from the groin access point got snared and pulled across to the upper side.
It is complicated but step-by-step it makes sense.
The stent balloooning just forces the thrombus open? The thrombus would essentially be squished between the stent and the vein wall, right? Do the remains of the thrombus cause any problems for endothelization?Now with the wire across the thrombus, i was able to deploy some stents, and then balloon them (not shown) against the vein wall to get a good seal.
I will take your word for it: a beautiful restoration of flow and diameter. It is amazing to take a completely blocked vein and make it work again.These images show an IVUS (center) to assure myself of a good apposition between stent and vein wall and nice IVUS (right) and venographic (left) images showing restoration of flow and diameter.
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
The turkey sandwich was great. I fare poorly when I skip meals!PointsNorth wrote:I thought that the turkey sandwich was pretty good. Altho it was 6pm and I hadn't eaten all day!
-
CD

- Family Elder
- Posts: 217
- Joined: Sun Dec 19, 2010 3:00 pm
- Location: USA
- Contact:
Re: DrSclafani answers some questions
Dr S. I am trying to find out the lifespan of stents. I have 3 Ev3 mesh titanium with nickle alloy stents placed in my left IJV. They do overlap each other from two procedures. Mine look similar to your above image with the stent/s. Mine may go even higher. I have a small neck. You can see and feel them. 
Cece said
CD
Cece said
What is your opinion please?I don't think we know yet what the lifespan of stents will be when placed in the jugulars. They may be subject to more movement stress here than in more stable areas of the body. I can remember one person reporting that they'd had a stent fracture but only that one person
CD
Last edited by CD on Mon Sep 26, 2011 8:50 pm, edited 1 time in total.
Where there is a will, there is a way. "HOPE"
CCSVI Procedure December 2010
CCSVI Procedure December 2010
-
pklittle

- Family Elder
- Posts: 341
- Joined: Sun Mar 07, 2010 3:00 pm
Re: DrSclafani answers some questions
Cece wrote:The turkey sandwich was great. I fare poorly when I skip meals!PointsNorth wrote:I thought that the turkey sandwich was pretty good. Altho it was 6pm and I hadn't eaten all day!
I like cookies better.
-
msfire

- Getting to Know You...
- Posts: 22
- Joined: Wed Sep 07, 2011 4:40 pm
- Location: Oshawa
Re: DrSclafani answers some questions
12 month check ups, I'm up for that, any reason to be part of Dr.S's reserch/passion is good for me.Cece wrote:I do not know which to be more excited about. But let's see!drsclafani wrote:1. 12 month followups of patients treated in 2011Cece wrote:Any other strategies or concepts on the docket to be explored in 2012?
2. Development of CCSVI Centers of Excellence at American Access Care
3. Dural sinus and deep cerebral vein pressure measurements with IVUS before and after treatment
4. A Bigger and Better Symposium
5. PwMS talent show at the symposium
6. Greater networking worldwide
7. publishing, publishing, publishing
* 12 month follow-ups! It must be difficult with patients that are not local.
* "CCSVI Centers of Excellence"...sounds promising!
* pressure measurements, which I think is similar to what Dr. Tucker was suggesting.
* Glad to hear there are still plans for a symposium next year, and a bigger & better one to boot!
* ok, publishing, publishing, publishing is my favorite
-
pelopidas
- Family Member
- Posts: 71
- Joined: Mon Sep 05, 2011 6:30 am
- Location: Greece
Re: Dural sinus are safe with DrS
Dr S.Cece wrote:Indeed, Disney World is full of characters, but there is only one character in the Brooklyn procedure room.drsclafani wrote:Lest the CCSVI world now spread a story that DrSclafani uses the Liberation Procedure as a recreational tool, let me end the rumor that the procedure room in Brooklyn, New York is my personal Disneyworld. I love m y work, but it ain't a game.
Plus, at Disney World, lots of food. In Brooklyn, no food until you make it to the turkey sandwich in the recovery room.
Also, at Disney World, the magic is pretend. Not so in the Brooklyn procedure room.
after the procedure you performed, i do not struggle along with all the things i have to do everyday
my life is fun and easy like Disney World
maybe this is what the rumor was all about, MY personal Disney World
getafix
-
Algis

- Family Elder
- Posts: 829
- Joined: Sat Nov 21, 2009 3:00 pm
- Location: XinYi District, Taipei City, , Taiwan
Re: DrSclafani answers some questions
On (6) "Greater networking worldwide" any chance of opening a branch clinic in Taiwan?
-
NZer1

- Family Elder
- Posts: 1624
- Joined: Thu Feb 18, 2010 3:00 pm
- Location: Rotorua New Zealand
Re: DrSclafani answers some questions
"Greater networking worldwide" any chance of opening a branch clinic in New Zealand? PleaseOn (6) "Greater networking worldwide" any chance of opening a branch clinic in Taiwan?
-
Algis
- Family Elder
- Posts: 829
- Joined: Sat Nov 21, 2009 3:00 pm
- Location: XinYi District, Taipei City, , Taiwan
Re: DrSclafani answers some questions
New-York / Taipei / Wellington is a nice flight 
Last edited by Algis on Mon Sep 26, 2011 9:00 pm, edited 1 time in total.
-
pklittle
- Family Elder
- Posts: 341
- Joined: Sun Mar 07, 2010 3:00 pm
Re: DrSclafani answers some questions
Yes, Yes,Yes !!!drsclafani wrote: 7. publishing, publishing, publishing
-
HappyPoet

- Family Elder
- Posts: 1414
- Joined: Thu Jul 09, 2009 2:00 pm
- Contact:
Re: DrSclafani answers some questions
DrS, it's wonderful that your rendezvous procedure was successful in helping to open the vein for stenting. Your success will give hope to those who lost their improvements when their IJVs closed.
What type of blockages are the most difficult to get through with guidewires: blood clots, intimal hyperplasia, or scar tissue? Did I miss any types of blockages? What factors contribute to how difficult a blockage is to get through with the guidewires? Also, is there any kind of rendezvousesque procedure available for the Azygos vein?
Regarding picture No. 8, what does the indentation on the left side in the upper stent signify and what factors might account for that portion of the stent not fully opening? Suddenly occurring to me is what about the other side of the stent that can't be seen? Can IRs see the outside of the vein/stent from all sides?
Edit: Do you have any images that show the tips of the two guidewires (one wire approaching from above the clot and the other wire approaching from below the clot) close to each other or meeting? Thanks!
What type of blockages are the most difficult to get through with guidewires: blood clots, intimal hyperplasia, or scar tissue? Did I miss any types of blockages? What factors contribute to how difficult a blockage is to get through with the guidewires? Also, is there any kind of rendezvousesque procedure available for the Azygos vein?
Regarding picture No. 8, what does the indentation on the left side in the upper stent signify and what factors might account for that portion of the stent not fully opening? Suddenly occurring to me is what about the other side of the stent that can't be seen? Can IRs see the outside of the vein/stent from all sides?
Edit: Do you have any images that show the tips of the two guidewires (one wire approaching from above the clot and the other wire approaching from below the clot) close to each other or meeting? Thanks!