Other summary. As introduction they say:
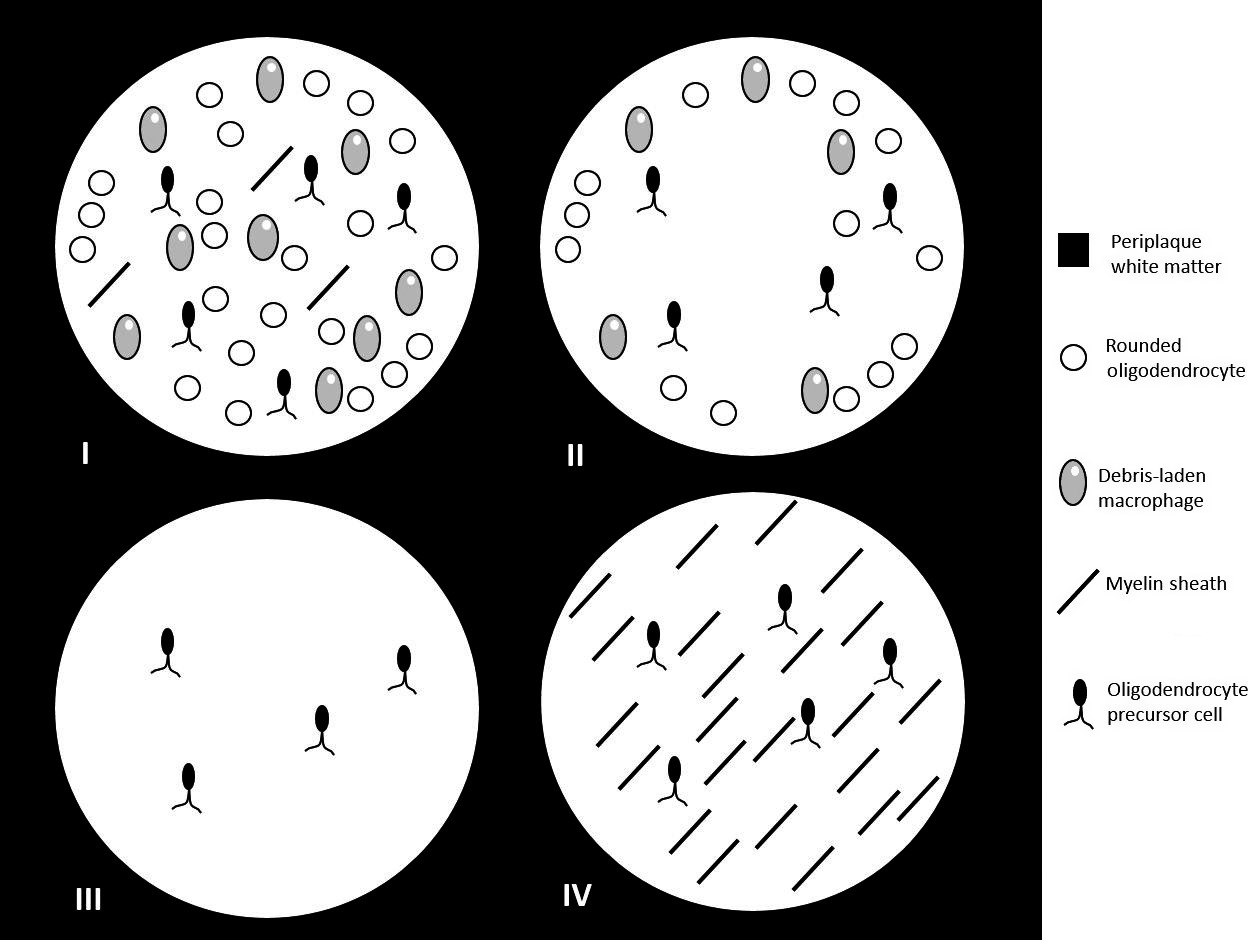
"Histopathological studies have demonstrated at least three different lesion patterns [...]. Pattern I show T cell and macrophage infiltration. Pattern II is defined by additional antibody and complement deposition Pattern III is characterized by distal oligodendrogliopathy [...].
These findings raise the possibility that MS, a diagnosis currently based mainly on phenotypical, namely clinical and radiological features, may in fact be a pathologically heterogeneous syndrome rather than a single disease entity. Importantly, two recent studies demonstrated intraindividual homogeneity and persistence of pattern I, II and III lesions over time further corroborating the notion that lesion pathology may rather define pathogenetically distinct entities than reflect stage-dependent processes in the development of lesions"
Pattern II and pattern III MS are entities distinct from pattern I MS: evidence from cerebrospinal fluid analysis
https://jneuroinflammation.biomedcentra ... 017-0929-z
Background: The diagnosis of multiple sclerosis (MS) is currently based solely on clinical and magnetic resonance imaging features. However, histopathological studies have revealed four different patterns of lesion pathology in patients diagnosed with MS, suggesting that MS may be a pathologically heterogeneous syndrome rather than a single disease entity.
Objective: The aim of this study was to investigate whether patients with pattern I MS differ from patients with pattern II or III MS with regard to cerebrospinal fluid (CSF) findings, especially with reference to intrathecal IgG synthesis, which is found in most patients with MS but is frequently missing in MS mimics such as aquaporin-4-IgG-positive neuromyelitis optica spectrum disorders and myelin oligodendrocyte glycoprotein-IgG-positive encephalomyelitis.
Methods: Findings from 68 lumbar punctures in patients who underwent brain biopsy as part of their diagnostic work-up and who could be unequivocally classified as having pattern I, pattern II or pattern III MS were analysed retrospectively.
Results: Oligoclonal bands (OCBs) were present in 88.2% of samples from pattern I MS patients but in only 27% of samples from patients with pattern II or pattern III MS (P < 0.00004); moreover, OCBs were present only transiently in some of the latter patients. A polyspecific intrathecal IgG response to measles, rubella and/or varicella zoster virus (so-called MRZ reaction) was previously reported in 60–80% of MS patients, but was absent in all pattern II or III MS patients tested (P < 0.00001 vs. previous cohorts). In contrast, the albumin CSF/serum ratio (QAlb), a marker of blood–CSF barrier function, was more frequently elevated in samples from pattern II and III MS patients (P < 0.002). Accordingly, QAlb values and albumin and total protein levels were higher in pattern II and III MS samples than in pattern I MS samples (P < 0.005, P < 0.009 and P < 0.006, respectively).
Conclusions: Patients with pattern II or pattern III MS differ significantly from patients with pattern I MS as well as from previous, histologically non-classified MS cohorts with regard to both intrathecal IgG synthesis and blood–CSF barrier function. Our findings strongly corroborate the notion that pattern II and pattern III MS are entities distinct from pattern I MS.
Other source:
Patterns I and II (specially pattern II) responsive to plasmapheresis. Pattern III unresponsive. This is just the last of several reports in this sense.
Differences in the Reponses to Apheresis Therapy of Patients With 3 Histopathologically Classified Immunopathological Patterns of Multiple Sclerosis
https://jamanetwork.com/journals/jamane ... irect=true
Abstract
Importance Plasma exchange and immunoadsorption are second-line apheresis therapies for patients experiencing multiple sclerosis relapses. Early active multiple sclerosis lesions can be classified into different histopathological patterns of demyelination. Pattern 1 and 2 lesions show T-cell– and macrophage–associated demyelination, and pattern 2 is selectively associated with immunoglobulin and complement deposits, suggesting a humoral immune response. Pattern 3 lesions show signs of oligodendrocyte degeneration. Thus it is possible that pathogenic heterogeneity might predict therapy response.
Objective To evaluate the apheresis response in relation to histopathologically defined immunopathological patterns of multiple sclerosis.
Design, Setting and Participants This single-center cohort study recruited 69 patients nationwide between 2005 and 2016. All included patients had a diagnosis of early active inflammatory demyelination consistent with multiple sclerosis; were classified into patterns 1, 2, or 3 based on brain biopsy analysis; and underwent apheresis treatments. Patients who had concomitant severe disease, neuromyelitis optica, or acute disseminated encephalomyelitis were excluded.
Main Outcomes and Measures The primary therapy outcome was a functionally relevant improvement of the relapse-related neurological deficit. Radiological and Expanded Disability Status Scale changes were secondary outcome parameters.
Results The mean (SD) age of patients was 36.6 (13.3) years; 46 of the 69 participants (67%) were female. Overall, 16 patients (23%) exhibited pattern 1 lesions, 40 (58%) had pattern 2 lesions, and 13 (19%) had pattern 3 lesions. A functional therapy response was observed in 5 of the 16 patients with pattern 1 disease (31%) and 22 of the 40 patients with pattern 2 disease (55%), but none of the 13 patients with pattern 3 disease exhibited improvement (pattern 2 vs 3 P < .001). Radiological improvements were found in 4 (25%), 22 (56%), and 1 (11%) of patients with patterns 1, 2, and 3, respectively. The respective rates of response measured by changes in Expanded Disability Status Scale scores were 25%, 40%, and 0%. Brainstem involvement was a negative predictive factor for the functional therapy response (logarithmic odds ratio [logOR], −1.43; 95% CI, −3.21 to 0.17; P = .03), while immunoadsorption (as compared with plasma exchange) might be a positive predictive factor (logOR, 3.26; 95% CI, 0.75 to 8.13; P = .01).
Conclusions and Relevance This cohort study provides evidence that the response to apheresis treatment is associated with immunopathological patterns. Patients with both patterns 1 and 2 improved clinically after apheresis treatment, but pattern 2 patients who showed signs of a humoral immune response benefited most. Apheresis appears unlikely to benefit patients with pattern 3 lesions.