No criticism was inferred.the retrospectoscope is a pain in the rear. I meant no criticisms of you or your doctor.
your days of pioneering are not yet completed
s
I also have no criticism of my doctors. Good to hear my pioneering days are not over
Speaking of that symposium, how was your IVUS talk received?drsclafani wrote:Well, now that the symposium is completed, i have had some time to think about interesting and informative cases.
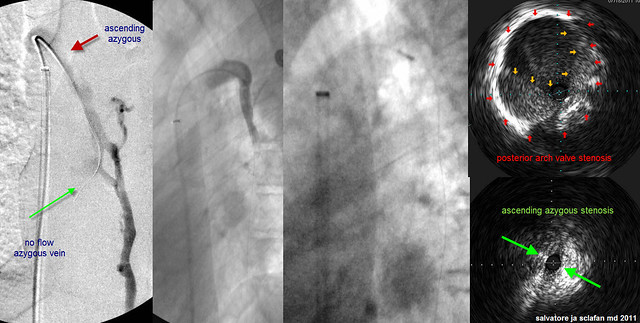
This is a particularly challenging azygous, isn't it? If it is hypoplastic or scarred down or recanalized, whatever it is that is keeping it small and not expanding on respiration, and it is disease of the vein rather than the more typical disease of the valve, then this vein was at risk of being overly damaged by being forced to the size it needed to be to accomodate the stent, then the extra blood flow due to the two compression syndromes is more needed or useful than it would be if this were a more simple valvular stenosis. (Although the patient had that as well.)drsclafani wrote:AZYGOUS VEIN
Since there is no obvious malformation or tissue change, it could be the result of the acquired posture after all these years of disease burden. Seen that way, it may not have great contribution to the overall situation and could be reduced by other means, ie exercising neck flexibility, adjusting sitting and sleeping posture, relaxing muscle tension. Thus, stenting might be too much.drsclafani wrote:So discussion number one. Should I have stented this vein?
Those are very intriguing comments.drsclafani wrote: i think that this problem needs to be corrected by better sleeping devices, perhaps improved pillows and re-education about positions of sleep....easier said than done. We must also understand that the position of the head for the procedure is not natural, only reproducible. Tilting the head only a little bit made a difference in flow and reflux.

there were someone who stated that there really wasnt any use for ivus, that it was an academic tool. However that person does not regularly use it, so i do not know what that opinion was based upon. Dr Zivadinov, whose group does use it, suggested that IVUS was probably the Gold Standard. Another opinion.Cece wrote:Speaking of that symposium, how was your IVUS talk received?drsclafani wrote:Well, now that the symposium is completed, i have had some time to think about interesting and informative cases.
You are too much cece, you put the question and the answer back to back. I like the way Dr Beggs explains things. he works on mathematic models using data published by others. He is so brilliant in his clarity as he explains the logic of the physical world.Did any of your colleagues bring up anything that made you think differently about any aspect of CCSVI?
Is Dr. Beggs really onto something? I've yet to work through his ideas, but I'm guessing it's worth the effort.
Dr. Siskin has weighed in here at TIMS on what he said at the conference about him seeing less positive outcomes and more risk of thrombosis if a patient has multiple procedures. Did the discussion at the doctors' days influence your thinking from what you said at the patient day, that as far as you knew so far, it was unlimited?
dear happypoetHappyPoet wrote:Thanks, DrS, for putting this case together. I can't believe how much I keep learning from you.drsclafani wrote:i think that this problem needs to be corrected by better sleeping devices, perhaps improved pillows and re-education about positions of sleep....easier said than done. We must also understand that the position of the head for the procedure is not natural, only reproducible. Tilting the head only a little bit made a difference in flow and reflux.
In what way(s) can pillows be improved?
Regarding "re-education about positions of sleep," what sleep positions do you recommend?
Thank you!
cece, what does it mean to be overly damaged? A vein that is completely obstructing is already overly damaged. Stents are an attempt to overcome the damage.Cece wrote:This is a particularly challenging azygous, isn't it? If it is hypoplastic or scarred down or recanalized, whatever it is that is keeping it small and not expanding on respiration, and it is disease of the vein rather than the more typical disease of the valve, then this vein was at risk of being overly damaged by being forced to the size it needed to be to accomodate the stent, then the extra blood flow due to the two compression syndromes is more needed or useful than it would be if this were a more simple valvular stenosis. (Although the patient had that as well.)drsclafani wrote:AZYGOUS VEIN
while not used in jugular veins, there are devices that can snip pieces of valves from within the vessel. There are also valve replacements.mo_en wrote:Dear Doctor, is there a way to cut out inert valve leaflets without getting involved in open surgery? What are the risks of such an intervention? Wouldn't this be an acceptable measure to deal with continuously restenosing veins, provided that all annulus issues have been resolved successfully?
I was making it easy on you, you are presumably still recovering from those 48 hour days.drsclafani wrote:You are too much cece, you put the question and the answer back to back. I like the way Dr Beggs explains things. he works on mathematic models using data published by others. He is so brilliant in his clarity as he explains the logic of the physical world.Cece wrote:Did any of your colleagues bring up anything that made you think differently about any aspect of CCSVI?
Is Dr. Beggs really onto something? I've yet to work through his ideas, but I'm guessing it's worth the effort.
I have been digesting his ideas since bologna.
Or he could still be recovering from my marathon procedure!I was making it easy on you, you are presumably still recovering from those 48 hour days.