I think brain cells begin to die after about 5 minutes without oxygen. So 8 minutes sounds risky unless there is enough redundancy in the veins to keep at least some blood flowing.Cece wrote:That is a frightening concern, MS_HOPE.MS_HOPE wrote:I agree about the eight minutes and six minutes, and have concerns about the back pressure that's being created, I would think, during the procedure itself, since the balloon cuts off flow during dilation. Am especially concerned because of a history of cerebral hemorrhages in my family, and my feeling that micro-hemorrhaging might be caused by the ballooning?
I don't know about the latter, but the former (does the balloon cut off flow during dilation) was asked in Dr. Sclafani's thread. I can't remember the answer exactly, was it that even if one outlet is blocked, all the other outlets (the other jugular, the verts, etc) are still in play?
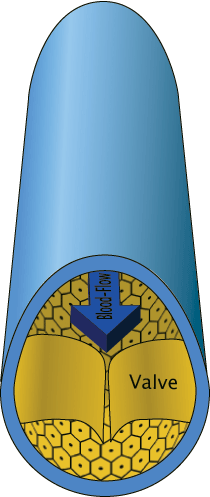
(An idiot's guide to) VALVES...?
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: (An idiot's guide to) VALVES...?
If the patient is not anticoagulated, any prolonged angioplasty is at risk of thrombosis. But eight minutes seems extreme to me.Cece wrote:Did you read in Dr. Sclafani's thread, about the "poor man's cutting balloon" where some docs will trap the guide wire against the vein and then inflate the balloon, using the guide wire to indent similar to how the cutting balloon indents?Johnson wrote:Doc mentioned cutting balloons, but they apparently don't come that big.
Eight minutes and six minutes seem like a really long time for ballooning! How long is normal?
I am disillusioned with the cutting balloon because the manufactured ones are too small and the home grown variety leave me disappointed so far. It seems to me that pressure is really important.
I would like to illustrate this with some images of some procedures using high pressure large diameter balloons. However, if you dont mind, i would like to post these on DrSclafani answers some questions so I can keep track of such illustrations.
the images show a variety of attempts to open a couple of tight stenoses of the valvular area, using medium and large sized balloons under lower pressures, a poor man's cutting balloon and finally a high pressure balloon at medium and high pressures. The stenosis finally broke at high pressure when all other manuevers failed. I am optimistic that this might be a solution for this particular problem
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
jugular flow is normally markedly diminished whenever one is in the upright position. I do not think that two minutes of inflation are going to cause microhemorrhage.Cece wrote:That is a frightening concern, MS_HOPE.MS_HOPE wrote:I agree about the eight minutes and six minutes, and have concerns about the back pressure that's being created, I would think, during the procedure itself, since the balloon cuts off flow during dilation. Am especially concerned because of a history of cerebral hemorrhages in my family, and my feeling that micro-hemorrhaging might be caused by the ballooning?
I don't know about the latter, but the former (does the balloon cut off flow during dilation) was asked in Dr. Sclafani's thread. I can't remember the answer exactly, was it that even if one outlet is blocked, all the other outlets (the other jugular, the verts, etc) are still in play?
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
jugular flow is normally markedly diminished whenever one is in the upright position. I do not think that two minutes of inflation are going to cause microhemorrhage.Cece wrote:That is a frightening concern, MS_HOPE.MS_HOPE wrote:I agree about the eight minutes and six minutes, and have concerns about the back pressure that's being created, I would think, during the procedure itself, since the balloon cuts off flow during dilation. Am especially concerned because of a history of cerebral hemorrhages in my family, and my feeling that micro-hemorrhaging might be caused by the ballooning?
I don't know about the latter, but the former (does the balloon cut off flow during dilation) was asked in Dr. Sclafani's thread. I can't remember the answer exactly, was it that even if one outlet is blocked, all the other outlets (the other jugular, the verts, etc) are still in play?
-
malden
During the procedure patient is not in upright position. And in supine position jugular pathway is dominant. So dominant pathway is blocked (not just narrowed) about 5 min, and that reflux and increased preasure is not a problem?!drsclafani wrote: jugular flow is normally markedly diminished whenever one is in the upright position. I do not think that two minutes of inflation are going to cause microhemorrhage.
First Zamboni's criteria for diagnostic CCSVI:
1. reflux in the internal jugular and vertebral veins > 0,88s
...
If only 1 sec of reflux is enough to diagnose Cronic Insuficiency, than 5 min (300 times longer time!) is much more dangerous for the brain too.
Maiden, wouldn't this depend on whether the demon is reflux or hypo perfusion? I think the key word is 'chronic' much like how a gentle stream of water can wear through a rock over time, but a temporary flood causes no long term damage. I often hang upside down on my inverter board for up to five minutes, with no apparent ill effect.
-
malden
I don't know, you tell me?Jugular wrote:Maiden, wouldn't this depend on whether the demon is reflux or hypo perfusion? I think the key word is 'chronic' much like how a gentle stream of water can wear through a rock over time, but a temporary flood causes no long term damage. I often hang upside down on my inverter board for up to five minutes, with no apparent ill effect.
Zamboni's followers does not measure perfusion over time... just 0,88 sec reflux in one vein ;)
Best regards, M
Let me answer this by not answering this. Instead I will outline 3 propositions:Malden wrote:I don't know, you tell me?Jugular wrote:Maiden, wouldn't this depend on whether the demon is reflux or hypo perfusion? I think the key word is 'chronic' much like how a gentle stream of water can wear through a rock over time, but a temporary flood causes no long term damage. I often hang upside down on my inverter board for up to five minutes, with no apparent ill effect.
Zamboni's followers does not measure perfusion over time... just 0,88 sec reflux in one vein ;)
Best regards, MaLden
1. There is a correlation between MS and venous stenoses;
2. Relieving the stenoses causes an improvement in MS symptoms;
3. CCSVI, reflux, hypo perfusion, etc.. are theories to explain 1 and 2.
Propositions 1 and 2 are based on observation. 3 is based on theory. A lot of researchers and doubters ... have attacked Zamboni on proposition 3. However, disproving 3 does not refute 1 and 2. This is a logical trap that some detracting neurologists have fallen into.
It takes a certain level of intelligence to identify a problem. A greater level is achieved by finding a solution. If 1 and 2 are true, then it becomes a challenge to find 3. If you don't accept 1 and 2 as proven facts then none of this will resonate with you and it's no use talking about 3.
...
Re: (An idiot's guide to) VALVES...?
Interesting, thanks. This would be the reason then for anticoagulating before the procedure, despite any potential risk of increased bleeding.drsclafani wrote:If the patient is not anticoagulated, any prolonged angioplasty is at risk of thrombosis.
I was looking for a place to put this image, I still love the title of this thread.
If the flaps work correctly, letting blood out and closing again to keep it out, it's a functional valve.
If it fails to let blood out, it's a nonfunctioning valve / outflow obstruction as seen in CCSVI.
Here is how things should be:
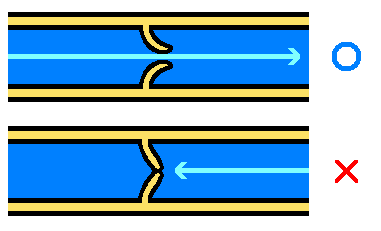
But in CCSVI, our jugulars look like the bottom picture, with the closed valve, all the time, because the valve is malformed and unable to open or close correctly.
I'm much less knowledgable then many of you however Cece's pictures of malformed valves functioning is pretty much what Dr. Arata (Pac Int) told us about. When he did my procedure the balloon was blown up enough so that I actually HEARD the crunch crunch crumch sound of the valve breaking up (or whatever the word would be). "Valves for Dummies" yep, I'd read that book.
-
MegansMom

- Family Elder
- Posts: 200
- Joined: Sun Aug 22, 2010 2:00 pm
- Location: Central FL ( near Ocala)
- Contact:
I love this thread, great pix Cece!
I'd like to add a few other pieces of info.
1. These veins are made of mesenchymal tissue, mesenchymal tissue responds to hormones, especially female hormones, the tissue is much more " stretchy" during pregnancy/ lactation. This may explain why there are less MS events during these times
2. Sheer stress and hypoxia both make the endothelium produce "endothelin 1" this "endothelin1" can cause fibrosis ( stiffness) and hypertrophy (thickening) of vessels (arteries and veins) especially valves. So from birth this may cause the veins/ valves to get worse CCSVI over time.
3. Endothelin1 is found in much higher levels in people with MS. It would be interesting to see if they could test if the level goes down after CCSVI angioplasty and normal cerebral venous outflow?
4.could a high level of Endothelin1 influence restenosis/ resumption of reflux after angioplasty?
5. There is so much to learn about all the chemicals/ reactions that occur in human blood vessels. we have only scratched the surface in our understanding of them. This is not so simple as fixing plumbing. Although believe me I support fixing the plumbing ASAP. arteries have gotten all of the attention, and veins need to catch up with intensive study.
I'd like to add a few other pieces of info.
1. These veins are made of mesenchymal tissue, mesenchymal tissue responds to hormones, especially female hormones, the tissue is much more " stretchy" during pregnancy/ lactation. This may explain why there are less MS events during these times
2. Sheer stress and hypoxia both make the endothelium produce "endothelin 1" this "endothelin1" can cause fibrosis ( stiffness) and hypertrophy (thickening) of vessels (arteries and veins) especially valves. So from birth this may cause the veins/ valves to get worse CCSVI over time.
3. Endothelin1 is found in much higher levels in people with MS. It would be interesting to see if they could test if the level goes down after CCSVI angioplasty and normal cerebral venous outflow?
4.could a high level of Endothelin1 influence restenosis/ resumption of reflux after angioplasty?
5. There is so much to learn about all the chemicals/ reactions that occur in human blood vessels. we have only scratched the surface in our understanding of them. This is not so simple as fixing plumbing. Although believe me I support fixing the plumbing ASAP. arteries have gotten all of the attention, and veins need to catch up with intensive study.
Cat (Catherine Somerville on FB)
MegansMom
My 35 yo daughter is newly dx 8/19/10 (had 12 symptoms)
Dx with Type A CCSVI- 1 IJV & double "candy wrapper" appearance of her Azygos
Venoplasty done Sept 21, 2010
Doing extremely well-
MegansMom
My 35 yo daughter is newly dx 8/19/10 (had 12 symptoms)
Dx with Type A CCSVI- 1 IJV & double "candy wrapper" appearance of her Azygos
Venoplasty done Sept 21, 2010
Doing extremely well-