Welcome!
DrSclafani answers some questions
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
This is a strong argument.drsclafani wrote:I have had the opportunity to re-treat a few patients who had been treated at sites in Asia, North America and Europe more than one year ago. The majority of the problems were either missed or underestimate obstructions or they were related to stents. Many other vessels were treated, yet on a venogram at the one year mark, it was often difficult to detect the sites of angioplasty. So where is the evidence that repeat procedures result in worse damage to these veins?
If the flow after the second procedure is equal to the flow after the first, then I don't think the answer is going to come from the IRs but from the neurology side of the equation.I have also seen patients have less improvements from a second procedure. We have to figure that one out.
I've always agreed with the thought that, as important as it is to find the right answers, it is more important to find the right questions.The more I know, the more I realize how much there is learn.
I see that happening with CCSVI. It is exciting.
-
pklittle

- Family Elder
- Posts: 341
- Joined: Sun Mar 07, 2010 3:00 pm
Dr. Sclafani,
This has already been brought up, but I need to ask again for clarity.
Dr's Siskin & Arata stress having just 1 and only 1 procedure if possible.
You have indicated that the number is unlimited to your knowledge. This is a huge difference in opinion.
Being that the pattern seems to be that at least some symptoms return to the patient over time, what's a person to do? It seems like there are at least two camps of thinking and the patient must choose on their own.
Can you help me understand?
Pam
This has already been brought up, but I need to ask again for clarity.
Dr's Siskin & Arata stress having just 1 and only 1 procedure if possible.
You have indicated that the number is unlimited to your knowledge. This is a huge difference in opinion.
Being that the pattern seems to be that at least some symptoms return to the patient over time, what's a person to do? It seems like there are at least two camps of thinking and the patient must choose on their own.
Can you help me understand?
Pam
-
NZer1

- Family Elder
- Posts: 1624
- Joined: Thu Feb 18, 2010 3:00 pm
- Location: Rotorua New Zealand
Thanks for your reply about the re treatment outcomes Dr..
I listened this morning to an interview of Dr Harris at Synergy. I got the impression that we are a long way from agreement on CCSVI.
I got the impression that Synergy had the belief that there have been 100% of the patients they have treated have 'CCSVI'. That those patients have CCSVI symptoms rather than MS symptoms and that those symptoms are the 'soft' symptoms such as cog fog/memory issues, heat intolerance, sleep issues, cold extremities. The MS symptoms are not changed, such as gait, balance, parathesia, spasticity 'hard symptoms'.
I am also of the belief that they have a policy of using MRI to Haacke as their guide to what they will treat and what they see as not requiring treatment rather than Zamboni Ultrasound.
After listening to the audio I would like to hear from you what you think is happening with the other providers (IRs). I get the impression that there are some that are not looking for all possible problems, with a view that only major problems are going to benefit (/effect the outcome on the table for) the patient. Is this what is happening in your opinion after the conference? Is there some who are looking only for instant symptom improvement, rather than let the body 'normalize and heal' itself with time?
(My personal view on this is that it will be an accumulation of total flow reduction that is going to be important in MS, and any other disease that is influenced by vascular problems. The disease has taken many years to develop any instant improvement would have to be questioned 'why'.)
I must add that I am totally impressed and in awe still by your ethos and persistence to leave no stone un-turned when you are helping us PwMS. When are you due for cloning?
Thank you.
Nigel
I listened this morning to an interview of Dr Harris at Synergy. I got the impression that we are a long way from agreement on CCSVI.
I got the impression that Synergy had the belief that there have been 100% of the patients they have treated have 'CCSVI'. That those patients have CCSVI symptoms rather than MS symptoms and that those symptoms are the 'soft' symptoms such as cog fog/memory issues, heat intolerance, sleep issues, cold extremities. The MS symptoms are not changed, such as gait, balance, parathesia, spasticity 'hard symptoms'.
I am also of the belief that they have a policy of using MRI to Haacke as their guide to what they will treat and what they see as not requiring treatment rather than Zamboni Ultrasound.
After listening to the audio I would like to hear from you what you think is happening with the other providers (IRs). I get the impression that there are some that are not looking for all possible problems, with a view that only major problems are going to benefit (/effect the outcome on the table for) the patient. Is this what is happening in your opinion after the conference? Is there some who are looking only for instant symptom improvement, rather than let the body 'normalize and heal' itself with time?
(My personal view on this is that it will be an accumulation of total flow reduction that is going to be important in MS, and any other disease that is influenced by vascular problems. The disease has taken many years to develop any instant improvement would have to be questioned 'why'.)
I must add that I am totally impressed and in awe still by your ethos and persistence to leave no stone un-turned when you are helping us PwMS. When are you due for cloning?
Thank you.
Nigel
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
pampklittle wrote:Dr. Sclafani,
This has already been brought up, but I need to ask again for clarity.
Dr's Siskin & Arata stress having just 1 and only 1 procedure if possible.
You have indicated that the number is unlimited to your knowledge. This is a huge difference in opinion.
Being that the pattern seems to be that at least some symptoms return to the patient over time, what's a person to do? It seems like there are at least two camps of thinking and the patient must choose on their own.
Can you help me understand?
Pam
i would not disagree that the goal should be to have one procedure. I am unaware of any angioplasties of any blood vessels that have a 0% restenosis rate. Certainly veins are well known for restenosis. If restenosis occurs in a patient who has had improvement that is lost, it seems to me that regaining that improvement is the primary goal of retreatment; otherwise, what was the purpose of doing the angioplasty in the first place.
i look at our goal as maximum improvement with minimum injury resulting is long term durability. Too small a balloon, too low a pressure, inadequate treatment but less risk of thrombosis or mural injury. too large a balloon disruption of the wall, complications
So we must balance risk against benefit, risk of injury versus benefit of the procedure. We are not there yet.
i am curious how these fine physicians came to their conclusion. Surely it is related to problems that have occured or inadequate treatment that resulted in restenosis. Their compromises seek the same solution, yet siskin is gentler and uses smaller balloon, arata is larger balloons and high pressure
for myself, i am seeking to develop a technique that is bold and gentle, based upon accurate and precise measurements that allow maximum dilatation with least amount of risk.
I think i am getting there.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
i have been saying that for over a year.NZer1 wrote:Thanks for your reply about the re treatment outcomes Dr..
I listened this morning to an interview of Dr Harris at Synergy. I got the impression that we are a long way from agreement on CCSVI.
I got the impression that Synergy had the belief that there have been 100% of the patients they have treated have 'CCSVI'.
i have been saying that publicly since march 2010.That those patients have CCSVI symptoms rather than MS symptoms and that those symptoms are the 'soft' symptoms such as cog fog/memory issues, heat intolerance, sleep issues, cold extremities.
i do not agree. Any one of many of my patients are most welcome to chime in. i have seen loss of foot drop, return of balance, color vision and vision clarity improved, numbness evaporate, wallwalkers ride bikes, hearing improve and incontinence go away.The MS symptoms are not changed, such as gait, balance, parathesia, spasticity 'hard symptoms'.
i think you are incorrect about how they utilize MRI.I am also of the belief that they have a policy of using MRI to Haacke as their guide to what they will treat and what they see as not requiring treatment rather than Zamboni Ultrasound.
I think there are some who still follow the recommendations of dr zamboni while others only look at the IJVeins and the Azygous. I think there are few who are looking at the connection between the dural sinuses and the jugular veins.After listening to the audio I would like to hear from you what you think is happening with the other providers (IRs). I get the impression that there are some that are not looking for all possible problems, with a view that only major problems are going to benefit (/effect the outcome on the table for) the patient. Is this what is happening in your opinion after the conference?
there may be some, i cant speak for anyone else, who are pleased to have immediate symptom improvement. I know I am. But healing of the disease called MS is not something that will be shown soon without large numbers of patients in studies.Is there some who are looking only for instant symptom improvement, rather than let the body 'normalize and heal' itself with time?
We wanat both but can measure only the symptoms at this moment.
What the IRs really want is to figure out the best way to perform the procedure. As I have said from the beginning, until we have that consensus or show that multiple techniques have comparable outcomes, we cannot measure long term effects with any reliability.
my view also. But our view is not important. it is the results that will sway the argument in the long run.(My personal view on this is that it will be an accumulation of total flow reduction that is going to be important in MS, and any other disease that is influenced by vascular problems. The disease has taken many years to develop any instant improvement would have to be questioned 'why'.)
thank you for the compliment. I am scheduled to be cloned on April 1, 2047 at the age of 100.I must add that I am totally impressed and in awe still by your ethos and persistence to leave no stone un-turned when you are helping us PwMS. When are you due for cloning? Thank you.
Nigel
hope to see you then
-
hope410
- Family Elder
- Posts: 125
- Joined: Mon Mar 08, 2010 3:00 pm
- Contact:
But yet Cece had a return of some symptoms a very short time after her first treatment with you and restenosis was confirmed on a repeat procedure just a few months after your first treatment in spite of the balance you are trying to achieve.drsclafani wrote:
for myself, i am seeking to develop a technique that is bold and gentle, based upon accurate and precise measurements that allow maximum dilatation with least amount of risk.
I think i am getting there.
Could you tell us why you think you're "getting there" with that kind of recurrence so soon after treatment? Is there REALLY a way to improve the odds of enduring patency the first time when even IVUS and precise dilatation that you are using doesn't prevent restenosis so soon after angioplasty?
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Well first of all, i never promised or predicted a single enduring therapy in the foreseeable future. I am looking to prolong the interval. In Zamboni's followup, patients had recurrence as early a couple of months; most restenosis occured between 8-14 months. So i cannot say (not having that much long term followup) that i have improved on his outcomes. Only time will prove that.hope410 wrote:But yet Cece had a return of some symptoms a very short time after her first treatment with you and restenosis was confirmed on a repeat procedure just a few months after your first treatment in spite of the balance you are trying to achieve.drsclafani wrote:
for myself, i am seeking to develop a technique that is bold and gentle, based upon accurate and precise measurements that allow maximum dilatation with least amount of risk.
I think i am getting there.
Could you tell us why you think you're "getting there" with that kind of recurrence so soon after treatment? Is there REALLY a way to improve the odds of enduring patency the first time when even IVUS and precise dilatation that you are using doesn't prevent restenosis so soon after angioplasty?
So Cece had six months treatment survival without recurrence and had small reductions in her improvements. I would not necessarily have treated her had she not been visiting from minnesota at the time for the symposium and if I had performed IVUS on her azygous vein when i treated her the first time. She and I agreed that repeating the diagnostic procedure to include IVUS was a reasonable approach. And a significant valvular abnormality was seen on that second treatment because of the use of IVUS. That seems like headway to me. No more will i rely upon only venography for analysis of the azygous vein. But surely this retreatment was done and counts as a retreatment. That is a fair question you ask.
What was exciting to me was the lack of evidence of long term injury to the veins that had been treated previously. In other words, there was no evidence of stenosis of the treated vein and no bulges and NO thrombosis.
Using empirically large balloons (18-20 for women and 18-24 for men as recommended at last years symposium by Dr Sinan) resulted in quite a few thromboses by all treating physicians. I am pleased that this has become rarer with a more precise IVUS based measurement of size of vein. I am quite pleased to have recognized that the stenosis was valvular rather than venous by using IVUS. This also makes a difference in how angioplasty is approached. And this will make a difference in the incidence of damage to the vein and subsequent stenosis.
Finally the differentiation of valves from septum to annulus stenosis that IVUS allows is going to help us to refine treatment depending upon those diagnoses. For sure there is more risk in dilating the annulus, and more likelihood of recurrence with septum.
so i do think i am getting there. I am not there yet
Last edited by drsclafani on Fri Jul 29, 2011 8:53 pm, edited 1 time in total.
-
phe
- Getting to Know You...
- Posts: 14
- Joined: Fri Oct 22, 2010 2:00 pm
Quote:
The MS symptoms are not changed, such as gait, balance, parathesia, spasticity 'hard symptoms'.
i do not agree. Any one of many of my patients are most welcome to chime in. i have seen loss of foot drop, return of balance, color vision and vision clarity improved, numbness evaporate, wallwalkers ride bikes, hearing improve and incontinence go away.
I am one of those persons who's hard symptom of spasticity has greatly decreased...so I am just jumping on board with that.
The interesting thing for me is this...transferring right from being in a w/chair to my bed at the end of the day, I can lie flat and read a book....no spastic leg up and down stuff. Yet, when I turn onto my left side and fall asleep-even if its only 20 min, that lack of spasticity disappears. I think some is postural-I have other back issues. But my osteopath is convinced some of this change is due to flow issues...what do I do to see if I can change that?
btw Dr Sclafani-when you did my surgery, you mentioned my scoliosis-its gone. My chiro and PTs cannot believe it...cool!
The MS symptoms are not changed, such as gait, balance, parathesia, spasticity 'hard symptoms'.
i do not agree. Any one of many of my patients are most welcome to chime in. i have seen loss of foot drop, return of balance, color vision and vision clarity improved, numbness evaporate, wallwalkers ride bikes, hearing improve and incontinence go away.
I am one of those persons who's hard symptom of spasticity has greatly decreased...so I am just jumping on board with that.
The interesting thing for me is this...transferring right from being in a w/chair to my bed at the end of the day, I can lie flat and read a book....no spastic leg up and down stuff. Yet, when I turn onto my left side and fall asleep-even if its only 20 min, that lack of spasticity disappears. I think some is postural-I have other back issues. But my osteopath is convinced some of this change is due to flow issues...what do I do to see if I can change that?
btw Dr Sclafani-when you did my surgery, you mentioned my scoliosis-its gone. My chiro and PTs cannot believe it...cool!
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
The real shame is that many people are having to self-pay. If a heart patient has angioplasty and then the arteries reclog, they don't have to pay, for a first procedure or a second procedure. Dr. Sclafani sees us gaining traction and he knows more than I do about how a procedure becomes mainstream and standard-of-care and, importantly, covered for everyone. It is encouraging, but in the meantime....in my case, I had partial restenosis in my LIJV but my right vein which had been severely blocked was fully patent at five months. The use of IVUS to precisely measure is mainly, in my mind, a protectant against oversizing. It succeeded: no thrombosis or intimal hyperplasia or collapse of the vein.Is there REALLY a way to improve the odds of enduring patency the first time when even IVUS and precise dilatation that you are using doesn't prevent restenosis so soon after angioplasty?
My best guess is that my LIJV restenosed very early. It had been 99% blocked by a monstrous valve leaflet. (MonStrous....) With the 60% restenosis, he described it as being from residual valve tissue.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
And while we are on the topic of restenosis and repeated angioplasties, allow me to share this case.
Patient has previously been treated by a well known and respected interventionalist. The first treatment revealed a right sided stenosis that was treated with a 12 mm balloon. The left side was thought to be an insignificant stenosis. There were improvements in several symptom complexes. The symptoms gradually returned over the next couple of months.
A second procedure done a few months after the first showed that the right IJV was not restenosed, but the left IJV was felt to be significantly stenosed and was treated with a 14 mm balloon. Again with clinical improvements and yet again with gradual deterioration back to baseline.
The woman then consulted me. Ultrasound showed residual valvular deformities and reflux only in the supine position. The test was equivocal. I expected no significant treatment options.
The right transverse sinus was catheterized and venography was performed. It showed no stenoses but there was reflux into the left dural sinuses and faster drainage into the left IJV than in the right IJV. However no definite stenosis was seen in the right internal jugular vein. IVUS was inconclusive and I went on to study the left side without any treatment on the right side.
Here is the left IJV imaging.

This venogram shows clearly about a 50% stenosis at the confluens. IVUS showed that this was a valvular stenosis. It is noteworthy that the area above the stenosis is not stretched and no bulges or flaps are seen. Clearly, there is no evidence of angioplasty injury. A 16 mm high pressure balloon was placed eccentrically at the stenotic segment and inflated to 14 atmospheres of pressure. The post angioplasty venogram has good flow and no stenosis.
The selection of balloon size is interesting. Below see the IVUS images.
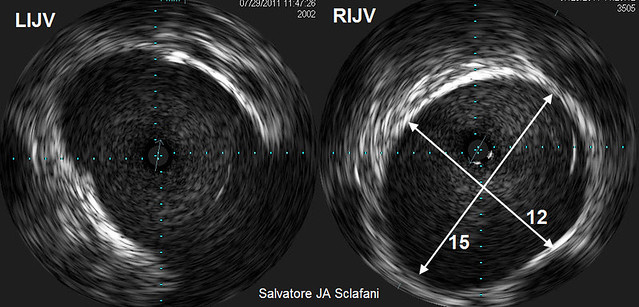
They show that the right vein is 15 mm by 12 mm and the left side is slightly larger. The balloons may just have been too small to effectively treat these stenoses. IVUS shows clearly that the 12 mm balloon on the right was way too small and that the 14 mm balloon is also too small on the left.
Perhaps the 16 mm balloon will be judged to be too small but i calculated that the 16 mm balloon is about 50% greater in surface area than the cross sectional area of these veins. I am dilating to 50-80% increase in cross sectional area measurement.
After treating the left side, I had second thoughts about not treating the right side. That vein just did not look right. While i didnt find a definite stenosis on venography further study of the IVUS showed bright signals in the vein. I wasnt sure those signals meant but they were inside the vein. I suspect they were webs or valves.
So I used the same 16 mm balloon to dilate the confluens of the right IJV.

The image on the left is a right dural venogram. Note the contrast in the left dural sinuses and in the left internal jugular vein. This is not normal. The area of the confluens (second image from the left) shows an irregular outline. I believe that some of this represents reflux into a collateral.
Angioplasty (third from the left) was performed. Upon nominal inflation two annular narrowings were identified. They went away with 14 Atm of pressure. The end result ( far right) looks pretty good).
Then on to the Azygous.
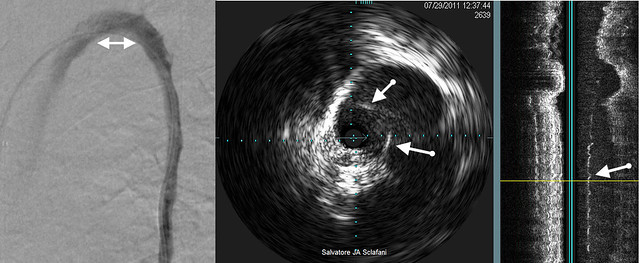
The venogram on the left shows a really nice open Azygous arch. No stenosis, no webs, no valves, nothin.
But IVUS shows a severely narrowed vein with about a 75% stenosis. The arrows point to intraluminal tissue that results in the narrowing. It is also visible on the sagittal reconstruction.
So is this really re-stenosis? We tend to assume that recurrence results from scar tissue caused by the angioplasty. Perhaps it is not. Perhaps it is incomplete dilatation resulting from too small a balloon. Perhaps stretching the narrowing is sufficient for short term clinical improvements but insufficient for a durable result.
So before we talk about restenosis, we need to be assured that the angioplasty was adequate.
Or course, all of this is interesting, but doesnt prove anything either. Whether a larger balloon is a solution is a longer term question that will be answered by clinical outcomes, not pictures. But i hope the pictures shed some light and provide food for thought.
Finally, there is no evidence that angioplasty causes injury. Again, there is NO evidence of vein wall injury after TWO angioplasties.
Patient has previously been treated by a well known and respected interventionalist. The first treatment revealed a right sided stenosis that was treated with a 12 mm balloon. The left side was thought to be an insignificant stenosis. There were improvements in several symptom complexes. The symptoms gradually returned over the next couple of months.
A second procedure done a few months after the first showed that the right IJV was not restenosed, but the left IJV was felt to be significantly stenosed and was treated with a 14 mm balloon. Again with clinical improvements and yet again with gradual deterioration back to baseline.
The woman then consulted me. Ultrasound showed residual valvular deformities and reflux only in the supine position. The test was equivocal. I expected no significant treatment options.
The right transverse sinus was catheterized and venography was performed. It showed no stenoses but there was reflux into the left dural sinuses and faster drainage into the left IJV than in the right IJV. However no definite stenosis was seen in the right internal jugular vein. IVUS was inconclusive and I went on to study the left side without any treatment on the right side.
Here is the left IJV imaging.
This venogram shows clearly about a 50% stenosis at the confluens. IVUS showed that this was a valvular stenosis. It is noteworthy that the area above the stenosis is not stretched and no bulges or flaps are seen. Clearly, there is no evidence of angioplasty injury. A 16 mm high pressure balloon was placed eccentrically at the stenotic segment and inflated to 14 atmospheres of pressure. The post angioplasty venogram has good flow and no stenosis.
The selection of balloon size is interesting. Below see the IVUS images.
They show that the right vein is 15 mm by 12 mm and the left side is slightly larger. The balloons may just have been too small to effectively treat these stenoses. IVUS shows clearly that the 12 mm balloon on the right was way too small and that the 14 mm balloon is also too small on the left.
Perhaps the 16 mm balloon will be judged to be too small but i calculated that the 16 mm balloon is about 50% greater in surface area than the cross sectional area of these veins. I am dilating to 50-80% increase in cross sectional area measurement.
After treating the left side, I had second thoughts about not treating the right side. That vein just did not look right. While i didnt find a definite stenosis on venography further study of the IVUS showed bright signals in the vein. I wasnt sure those signals meant but they were inside the vein. I suspect they were webs or valves.
So I used the same 16 mm balloon to dilate the confluens of the right IJV.
The image on the left is a right dural venogram. Note the contrast in the left dural sinuses and in the left internal jugular vein. This is not normal. The area of the confluens (second image from the left) shows an irregular outline. I believe that some of this represents reflux into a collateral.
Angioplasty (third from the left) was performed. Upon nominal inflation two annular narrowings were identified. They went away with 14 Atm of pressure. The end result ( far right) looks pretty good).
Then on to the Azygous.
The venogram on the left shows a really nice open Azygous arch. No stenosis, no webs, no valves, nothin.
But IVUS shows a severely narrowed vein with about a 75% stenosis. The arrows point to intraluminal tissue that results in the narrowing. It is also visible on the sagittal reconstruction.
So is this really re-stenosis? We tend to assume that recurrence results from scar tissue caused by the angioplasty. Perhaps it is not. Perhaps it is incomplete dilatation resulting from too small a balloon. Perhaps stretching the narrowing is sufficient for short term clinical improvements but insufficient for a durable result.
So before we talk about restenosis, we need to be assured that the angioplasty was adequate.
Or course, all of this is interesting, but doesnt prove anything either. Whether a larger balloon is a solution is a longer term question that will be answered by clinical outcomes, not pictures. But i hope the pictures shed some light and provide food for thought.
Finally, there is no evidence that angioplasty causes injury. Again, there is NO evidence of vein wall injury after TWO angioplasties.
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
While Dr. Sclafani is very good at explaining these procedures on a level we can understand, I would not argue that he is perfect...surely there are comments or questions?
And Dr. Sclafani, if you have the time, what were your thoughts on this question from the other day?
And Dr. Sclafani, if you have the time, what were your thoughts on this question from the other day?
vlpg wrote:Dr Sclafani thank you for enerything you do for us.I was very pleased when i read that narrowing renal vein affects CCSVI.
I did the procedure in June.I started to deteriorate dramatically although my ultrasound is good.For this deterioration can be responsible other veins except jugular and azygous veins?
Thank you.
vlpg wrote:Nice to meet you!Cece,thank you for your reply. I suffer from ms 6 years in relapsing form. I have several relapses 17 until now with many symptoms. Last year i had the procedure 3 failured times. The vascular surgeon who made the procedures had not enough experience to this procedure. Although, after my 1st procedure I saw many improvements for a month but then i became worse.
I made an other ultrasound to a radiologist who is the best here in Greece and takes part to a clinic trial. He found that in left jugular vein i have valve promblem(my valve didn't move and i had a diaphragm) in right jugular i had a diaphragm ,and my azygous seemed that had also blood flow problem.He reffered me to another interventional radiologist to redo the procedure.They have spent almost 2 months since then.I did ultrasound 2 times after the procedure and it was obviously that it was good. What concerns me is that i become worse. So i wonder whether other veins are likely to cause this deterioration.
-
HappyPoet

- Family Elder
- Posts: 1414
- Joined: Thu Jul 09, 2009 2:00 pm
- Contact:
Hi Dr. Sclafani,
Thank you, DrS!drsclafani wrote:And while we are on the topic of restenosis and repeated angioplasties, allow me to share this case.
Patient has previously been treated by a well known and respected interventionalist. The first treatment revealed a right sided stenosis that was treated with a 12 mm balloon. The left side was thought to be an insignificant stenosis. There were improvements in several symptom complexes. The symptoms gradually returned over the next couple of months.
A second procedure done a few months after the first showed that the right IJV was not restenosed, but the left IJV was felt to be significantly stenosed and was treated with a 14 mm balloon. Again with clinical improvements and yet again with gradual deterioration back to baseline.
The woman then consulted me. Ultrasound showed residual valvular deformities and reflux only in the supine position. The test was equivocal. I expected no significant treatment options.
The right transverse sinus was catheterized and venography was performed. It showed no stenoses but there was reflux into the left dural sinuses and faster drainage into the left IJV than in the right IJV. However no definite stenosis was seen in the right internal jugular vein. IVUS was inconclusive and I went on to study the left side without any treatment on the right side.
I'm puzzled by the reflux of contrast into the L-DS after venography of the R-TS. What path did the contrast take and what accounts for this reflux? Do you have video of this as it's happening that you can show (maybe youtube)?
Here is the left IJV imaging.
This venogram shows clearly about a 50% stenosis at the confluens. IVUS showed that this was a valvular stenosis. It is noteworthy that the area above the stenosis is not stretched and no bulges or flaps are seen. Clearly, there is no evidence of angioplasty injury. A 16 mm high pressure balloon was placed eccentrically at the stenotic segment and inflated to 14 atmospheres of pressure. The post angioplasty venogram has good flow and no stenosis.
So, at this point in time, all appears well with the once-treated R-IJV. The once-treated L-IJV venous wall, though, appears intact, as if only temporarily stretched with too small a balloon--which accounts for both the temporary improvement in symptoms and no permanent injury to the vein wall above the stenosis. Could it be, though, that the vein wall, itself, was never dilated, that the balloon shoulder had been placed against just the valvular stenosis and not the vein wall at all, eccentrically ala Sclafani?
How does the number of times the balloon is inflated and the length of time the balloon is inflated fit into the overall equation that also includes the atmospheres of pressure used/required and the size of balloon chosen, ala Sclafani IVUS Balloon-sizing Method discussed below?
The selection of balloon size is interesting. Below see the IVUS images.
They show that the right vein is 15 mm by 12 mm and the left side is slightly larger. The balloons may just have been too small to effectively treat these stenoses. IVUS shows clearly that the 12 mm balloon on the right was way too small and that the 14 mm balloon is also too small on the left.
Perhaps the 16 mm balloon will be judged to be too small but i calculated that the 16 mm balloon is about 50% greater in surface area than the cross sectional area of these veins. I am dilating to 50-80% increase in cross sectional area measurement.
If a patient wanted a conservative procedure, is balloon sizing an area where a patient could ask for you to dilate only to a 50% increase in cross sectional area measurement as opposed to 80%?
After treating the left side, I had second thoughts about not treating the right side. That vein just did not look right. While i didnt find a definite stenosis on venography further study of the IVUS showed bright signals in the vein. I wasnt sure those signals meant but they were inside the vein. I suspect they were webs or valves.
So I used the same 16 mm balloon to dilate the confluens of the right IJV.
Where did you place the shoulder of the balloon? Was there a valve at the confluens? Was this decision difficult?
The image on the left is a right dural venogram. Note the contrast in the left dural sinuses and in the left internal jugular vein. This is not normal. The area of the confluens (second image from the left) shows an irregular outline. I believe that some of this represents reflux into a collateral.
Angioplasty (third from the left) was performed. Upon nominal inflation two annular narrowings were identified. They went away with 14 Atm of pressure. The end result ( far right) looks pretty good).
Again, I'm puzzled. Will this angioplasty stop blood from flowing/refluxing down the L-DS and L-IJV?
By "annular narrowings," do you mean the two areas seen had an actual annulus with no valve flaps? Was there a "pop" heard when the annular narrowings went away?
Then on to the Azygous.
The venogram on the left shows a really nice open Azygous arch. No stenosis, no webs, no valves, nothin.
But IVUS shows a severely narrowed vein with about a 75% stenosis. The arrows point to intraluminal tissue that results in the narrowing. It is also visible on the sagittal reconstruction.
This shows the value of IVUS.
I honestly don't see anything on the sagital reconstruction where the arrow is pointing near the thin, green horizontal line. What does the large shift in signal represent far above the arrow?
So is this really re-stenosis? We tend to assume that recurrence results from scar tissue caused by the angioplasty. Perhaps it is not. Perhaps it is incomplete dilatation resulting from too small a balloon. Perhaps stretching the narrowing is sufficient for short term clinical improvements but insufficient for a durable result.
So before we talk about restenosis, we need to be assured that the angioplasty was adequate.
This makes sense; how does an IR tell the difference between thrombosis, and/or intimal hyperplasia, and/or valvular or intraluminal tissue that is either not staying pressed into the vein wall or is a defect?
Or course, all of this is interesting, but doesnt prove anything either. Whether a larger balloon is a solution is a longer term question that will be answered by clinical outcomes, not pictures. But i hope the pictures shed some light and provide food for thought.
All of this is VERY interesting.
Finally, there is no evidence that angioplasty causes injury. Again, there is NO evidence of vein wall injury after TWO angioplasties.
Please forgive my cogfog, but I don't get this--what about restenosis?
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Yes, it is possible to worsen if all problems are not corrected. I have now seen a few patients who did not until after the renal vein stenosis was corrected. The left renal vein is a serious concern because of the very high flow in the vein and the nature of the collaterals lead the blood t0he azygous system. The May thurner syndrome, seen in 5% of healthy controls is a similar problem that should be looked for.Cece wrote:While Dr. Sclafani is very good at explaining these procedures on a level we can understand, I would not argue that he is perfect...surely there are comments or questions?
And Dr. Sclafani, if you have the time, what were your thoughts on this question from the other day?
I have not found the post procedure ultrasound to be a perfect correlation to clinical symptoms of the patient. Sometimes reflux is seen yet the patient is having a wonderful improvement. Also It is possible that restenosis or some problem with the vein may occur in the absence of abnormal ultrasound.vlpg wrote:Dr Sclafani thank you for enerything you do for us.I was very pleased when i read that narrowing renal vein affects CCSVI.
I did the procedure in June.I started to deteriorate dramatically although my ultrasound is good.For this deterioration can be responsible other veins except jugular and azygous veins?
Thank you.
If you are "dramatically deteriorating" after the treatment, I would suggest that another venogram is warranted.
vlpg wrote: I suffer from ms 6 years in relapsing form. I have several relapses 17 until now with many symptoms. Last year i had the procedure 3 failured times. The vascular surgeon who made the procedures had not enough experience to this procedure. Although, after my 1st procedure I saw many improvements for a month but then i became worse.
I made an other ultrasound to a radiologist who is the best here in Greece and takes part to a clinic trial. He found that in left jugular vein i have valve promblem(my valve didn't move and i had a diaphragm) in right jugular i had a diaphragm ,and my azygous seemed that had also blood flow problem.He reffered me to another interventional radiologist to redo the procedure.They have spent almost 2 months since then.I did ultrasound 2 times after the procedure and it was obviously that it was good. What concerns me is that i become worse. So i wonder whether other veins are likely to cause this deterioration.