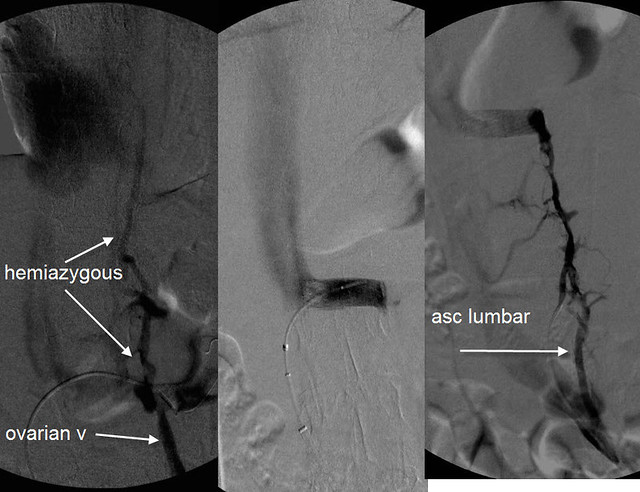
drsclafani wrote:RNutcracker syndrome may be a clinically occult problem in healthy patients but in patients with compromised outflow of the azygous vein, additional blood flow enters the vertebral plexus and the spinal veins. thus compounds the CCSVI resulting from the stenoses of the right and left IJV and the azygous vein.
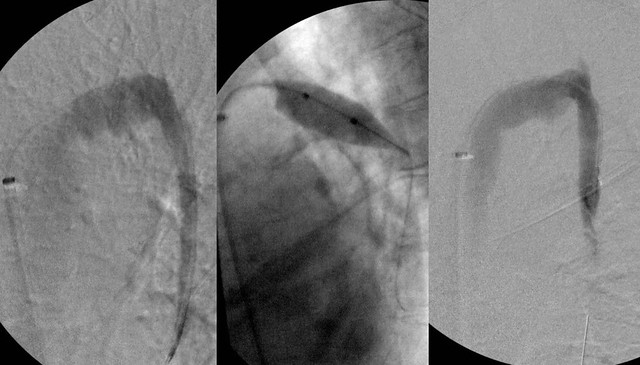
But these images of the renal vein and collaterals were taken after the azygous was treated, correct? So even after the azygous was treated, it appears that there is contrast going into the ascending lumbars? By the time you got to this part of the procedure, the patient had corrected flow in the jugulars and in the azygous. It's interesting.
After the competion of the procedure the patient upon questioning volunteered information regarding chronic pain near the left ovary that was, to her reminiscent of pain in the ovary during menstruation. (she is post menopausal). Thus i believe that she has pelvic congestion caused by reflux of renal vein blood into her ovarian vein resulting from the nutcracker syndrome.
mystery solved....
It will be interesting to see whether her ovarian symptoms improve now that the renal vein has been opened. However the high flow down the ovarian vein has resulted in incompetence of the valves of her ovarian vein and she may not get relief without treatment of the ovarian vein syndromed.
The treatment is blockade of the ovarian vein from the flow in the renal vein by embolization.
Ovarian vein valves! That was helpful to explain it. High flow in the wrong direction would indeed be detrimental to the function of valves meant to control flow in the opposite direction. Embolization would seal off the vein to the incoming wrong-way flow from the renal vein, allowing things to flow the right way again, even without working valves.
whew, I worked through this case, next case please!

There was a whole month without them, you know. Such hardship.
(But no pressure, much respect for your limited time, etc!)