Which of the symptom list will be changed by what you achieve?
And actually I mean to say thank you for spending the time you currently have to keeping pushing the envelope.
Any luck with finding people eg Neuros and Radiology to work along side what you are unearthing?
The changes that are happening have to be understood, and the there is so much more learning to come.
Is there any response from Radiologists and Neurology about the outcomes of the changes you have achieved?
Is there any one looking at why we PwMS have such varying symptoms and yet such a tight dx?
What is happening to the peripheral group of us who have a blend of symptoms that fall in many disease groupings that Radiology and Neurology have not found the time to look into. Money can be made in management of symptoms but not in defining diseases!
Had to have a bleat, thanks Sal you are moving Mountains,
Nigel
DrSclafani answers some questions
-
NZer1

- Family Elder
- Posts: 1624
- Joined: Thu Feb 18, 2010 3:00 pm
- Location: Rotorua New Zealand
-
NZer1
- Family Elder
- Posts: 1624
- Joined: Thu Feb 18, 2010 3:00 pm
- Location: Rotorua New Zealand
Re: DrSclafani answers some questions
The reason for my bleat which is totally not directed at you Sal, is that I have been shown a symptom list that may cover many of us PwMS and yet there is no clarity as to which area we each need to pursue.
http://chiarione.org/symptoms.html
And in essence why do patients need to dx them selves?
Most of these symptoms are cross overs for so many of Neurology's caption of MS based on a theory of Autoimmunity.
My frustration is flooding over as you are aware, and no doubt your own has been for some time. Do we look at fixing what is broken then look the outcome? It seems so bizarre that we have to confront this in this way! I am now understanding why Mike Arata is approaching his treatments and media outcomes the way he is.
I'll shut up, have a meal and do what people call sleep, (fill time until the sun rises because my body has other ideas).
Nigel
http://chiarione.org/symptoms.html
And in essence why do patients need to dx them selves?
Most of these symptoms are cross overs for so many of Neurology's caption of MS based on a theory of Autoimmunity.
My frustration is flooding over as you are aware, and no doubt your own has been for some time. Do we look at fixing what is broken then look the outcome? It seems so bizarre that we have to confront this in this way! I am now understanding why Mike Arata is approaching his treatments and media outcomes the way he is.
I'll shut up, have a meal and do what people call sleep, (fill time until the sun rises because my body has other ideas).
Nigel
-
NHE

- Volunteer Moderator
- Posts: 6477
- Joined: Sat Nov 20, 2004 3:00 pm
- Contact:
Re: DrSclafani answers some questions
Not yet. Just thought that I would mention that there are abundant typo's where a lower case l was apparently substituted for a lower case i. There's also a couple of other letters that have been replaced by an l.drsclafani wrote:Any questions?
It's great to read that IVUS has improved the safety of the procedure
NHE
-
dlynn
- Family Elder
- Posts: 229
- Joined: Thu Jul 28, 2011 2:00 pm
Re: DrSclafani answers some questions
Hi Dr. Sclafani, I've been reading alot about leg veins possibly being involved as part of the problem with walking.
I've had an US of my legs (veins) and they are fine, no problems. I've had 3 procedures, all 3 times my Azygous and lIJV were treated.
My rIJV was treated the first and second procedure and remained open. An US 5 mos. ago showed good flow in both IJV's.
But why do my legs continue to get weak and unsteady?
Would you suggest I have other veins looked at. I'm so frustrated, I'm in PT (working on balance and core strength).
I'm not sure if a fourth procedure would help as I don't know if my Azygous has restenosed.
Thank you for your thoughts.
God bless!!
I've had an US of my legs (veins) and they are fine, no problems. I've had 3 procedures, all 3 times my Azygous and lIJV were treated.
My rIJV was treated the first and second procedure and remained open. An US 5 mos. ago showed good flow in both IJV's.
But why do my legs continue to get weak and unsteady?
Would you suggest I have other veins looked at. I'm so frustrated, I'm in PT (working on balance and core strength).
I'm not sure if a fourth procedure would help as I don't know if my Azygous has restenosed.
Thank you for your thoughts.
God bless!!
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
They are just Google OCR errors.Besides, I am an iconoclastic egalitarian who does not believe that there should be distinction between upper and lower case letters. Everyone of them should be considered equal.NHE wrote:Not yet. Just thought that I would mention that there are abundant typo's where a lower case l was apparently substituted for a lower case i. There's also a couple of other letters that have been replaced by an l.drsclafani wrote:Any questions?
It's great to read that IVUS has improved the safety of the procedure
NHE
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
munchkin
- Family Elder
- Posts: 312
- Joined: Fri Apr 01, 2011 2:00 pm
- Location: Canada
- Contact:
Re: DrSclafani answers some questions
Dr. S
Thank you for your work with IVUS, what an amazing reduction in vein injury.
Based on the reduction of trauma to the vein using IVUS have you been able to recommend parameters on sizing of balloons based on the corresponding vein size?
Will this information help establish a set of guidelines for treatment protocols?
Thank you for your work with IVUS, what an amazing reduction in vein injury.
Based on the reduction of trauma to the vein using IVUS have you been able to recommend parameters on sizing of balloons based on the corresponding vein size?
Will this information help establish a set of guidelines for treatment protocols?
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
Last edited by Cece on Wed Dec 07, 2011 3:11 pm, edited 1 time in total.
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
When you say that 82% had bilateral angioplasty, was that 82% of 150 patients or 82% of the 93% who had angioplasty of the IJVs? It's a high percentage for bilateral IJV stenoses.drsclafani wrote:Any questions?
I like the statement that CCSVI stenoses are different than stenoses caused by thrombosis, recanalization, scarring, tumor encasement and access intimal hyperplasia. Defining what CCSVI is not is as important as defining what CCSVI is.
I think we can agree that complete distension of such obstructions is a worthy goal if it is correct that recoil is likely if an obstruction is incompletely distended, and if complete distension can be safely achieved.We sought to determine the balloon sizes and pressures that were necessary to attain complete distension of IJV obstructions due to CCSVI.
Why was >50% used as the percentage? I seem to remember conversations here about a blockage in a vein having a greater effect on flow than a blockage in an artery, and therefore lower percentages such as 30% or 40% might require treatment?Angioplasty was based upon venographic findings such as stenosis >50%, stasis, reflux, collaterals or upon intravascular ultrasound (IVUS) findings, such as cross sectional area stenoses (CSA)>50%, immobile valves, septum, membranes or webs.
You mention septums, I am curious: the Cleveland Clinic autopsy study found a significant number of septums in the IJVS of MS patients. I would've expected fewer septums since we don't hear much about them. In what percentage of your patients have you found septums in the IJVs? Can a septum be clearly distinguished from a valve, or from a membrane or web, on IVUS? How have septums been responding to treatment? Any ideas of how to improve treatment of septums?
It is interesting too that this breaks down what can be seen on venography: stenosis>50%, stasis, reflux or collaterals. (I remember you showing me the stasis in my left jugular, when I was there in July.) This is compared to what can be seen on IVUS: stenoses>50% as measured by cross sectional area, immobile valves, septum, membranes or webs. Stasis and reflux and collaterals are not listed as being seen on IVUS? But CSA and the intraluminal abnormalities (valves, septums, membranes, webs) are not listed as being seen on venography. Ok, no question there, just working through the differences between the IVUS and venography.
If these are Atlas balloons, the burst pressure is quite high, around 30 atm? Then burst pressure isn't a factor, since your highest pressure was 24 atm, and you went up in pressure until the waist was eliminated without recoil. I don't think we've had any other abstracts showing the use of high pressure balloons in CCSVI. If a high pressure balloon were to damage the vein wall, this would not be immediately known, but would show up over a few weeks or months, correct? I would like for this abstract to be demonstrative of safety of high pressure balloons, because I've heard both sides of the discussion on high pressure balloons, but if any damage isn't immediate, then this does not serve that purpose.lnflation endpoints were elimination of balloon waist without recoil or exceeding rated burst pressure.
What is the difference between a dissection and a perforation?
A strong statement here. Complications reduced from 16% to 1.3%, with the use of IVUS! Have you shared this with other IRs? What has the response been? Is this influencing other IRs to use IVUS, and if not, what would it take to influence IRs into using IVUS in CCSVI? As a patient advocate, I would like to see the safest, best methods adopted. There is no reason to take a 16% risk of damage of thrombosis or dissection of these precious veins, if the risk could be 1%.All but one dissection and one thrombosis occurred prior to using IVUS CSA for balloon selection. Complication rate of 16% using visual estimation was reduced to 1.3% using IVUS CSA measurements.
The alternative to high pressure is to go up in balloon size or to accept an endpoint with residual waisting or recoil. In this abstract, you did not explore the alternative of going up in balloon size, which you really can't do, if you belive that will lead to thrombosis or damage (by a combination of oversizing balloons and high pressure). I am not sure that the abstract supports the conclusion that high pressure is required. Nor do we know if complete dilation is superior to incomplete dilation, in terms of long-term results and safety, although it seems logical.Conclusion :
1. Hlgh pressures are requlred to completely dilate the lesions of CCSVI.
-
pelopidas
- Family Member
- Posts: 71
- Joined: Mon Sep 05, 2011 6:30 am
- Location: Greece
Re: DrSclafani answers some questions
I think that CCSVI treatment (like any other treatment) should be about:drsclafani wrote:SIR Abstract
Any questions?
There were three balloon ruptures, two occurred during removal from the sheath.There were three dissections, two perforations and ten thromboses (6.3% of treated veins). All but one dissection and one thrombosis occurred prior to using IVUS CSA for balloon selection. Complication rate of 16% using visual estimation was reduced to 1.3% using IVUS CSA measurements.
Conclusion :
1. Hlgh pressures are requlred to completely dilate the lesions of CCSVI.
2. IVUS reduces rlsk of veln lnjury during angioplasty.
1.safety
2.success
If IVUS is the only way to achieve both of them, is there any special reason that all IRs do not use it?
getafix
-
CD

- Family Elder
- Posts: 217
- Joined: Sun Dec 19, 2010 3:00 pm
- Location: USA
- Contact:
Re: DrSclafani answers some questions
I agree, safety and success should be the end result.pelopidas wrote:I think that CCSVI treatment (like any other treatment) should be about:drsclafani wrote:SIR Abstract
Any questions?
There were three balloon ruptures, two occurred during removal from the sheath.There were three dissections, two perforations and ten thromboses (6.3% of treated veins). All but one dissection and one thrombosis occurred prior to using IVUS CSA for balloon selection. Complication rate of 16% using visual estimation was reduced to 1.3% using IVUS CSA measurements.
Conclusion :
1. Hlgh pressures are requlred to completely dilate the lesions of CCSVI.
2. IVUS reduces rlsk of veln lnjury during angioplasty.
1.safety
2.success
If IVUS is the only way to achieve both of them, is there any special reason that all IRs do not use it?
I think Dr Sclafani said, at one time, that the IVUS machine/ equipment cost is very highly priced, and that the disposable catheters with camera is very expensive also, all adding to the cost of the CCSVI procedure. IMO, that is why many IR's are not using IVUS.
CD
Where there is a will, there is a way. "HOPE"
CCSVI Procedure December 2010
CCSVI Procedure December 2010
-
munchkin
- Family Elder
- Posts: 312
- Joined: Fri Apr 01, 2011 2:00 pm
- Location: Canada
- Contact:
Re: DrSclafani answers some questions
Dr. S
Forgive me if this has been asked before.
Have you had more of your treated patients reported improvements since you started using IVUS?
Thank you.
Forgive me if this has been asked before.
Have you had more of your treated patients reported improvements since you started using IVUS?
Thank you.
-
MrSuccess
- Family Elder
- Posts: 922
- Joined: Fri Sep 18, 2009 2:00 pm
Re: DrSclafani answers some questions
I find the " nutcracker " of great interest . Is it possible to navigate such a tight pathway and not inflict internal vein wall damage ? Does 20 mins. sound like plausible time frame to enter and explore the suspected vein pathway's of pwMS ?
Am I reading it correctly ..... that the procedure is often several HOURS in duration ?
Keep up the good work , dear doctor.
MrSuccess
Am I reading it correctly ..... that the procedure is often several HOURS in duration ?
Keep up the good work , dear doctor.
MrSuccess
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
What a great weekend this would be for a case report! 
Or is there nothing new under the sun to show us?
(I understand too if time is short and duties long.)
Or is there nothing new under the sun to show us?
(I understand too if time is short and duties long.)
-
pelopidas
- Family Member
- Posts: 71
- Joined: Mon Sep 05, 2011 6:30 am
- Location: Greece
Re: DrSclafani answers some questions
I had a terrible chronic neck pain and occipital headache (in the back of my head) for the past 7-8 years.
MRI showed some mildly prolapsed cervical disk, so i thought i would live with it forever. I was having physiotherapy and i was taking pain killers almost every second day.
Then, 6 months ago (6/10/2011) i had my angioplasty procedure.
One month later i was talking to Dr Sclafani about the great improvements i already had. I mentioned that my neck pain was unexpectedly disappeared. He replied only "Ah, it was the spasm!"
I found what he meant:
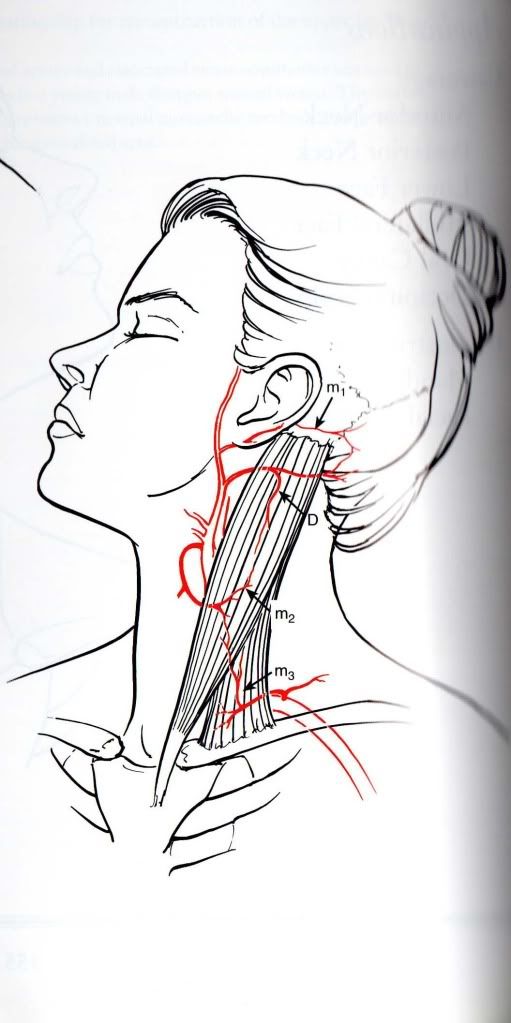
http://i1129.photobucket.com/albums/m51 ... stoid1.jpg
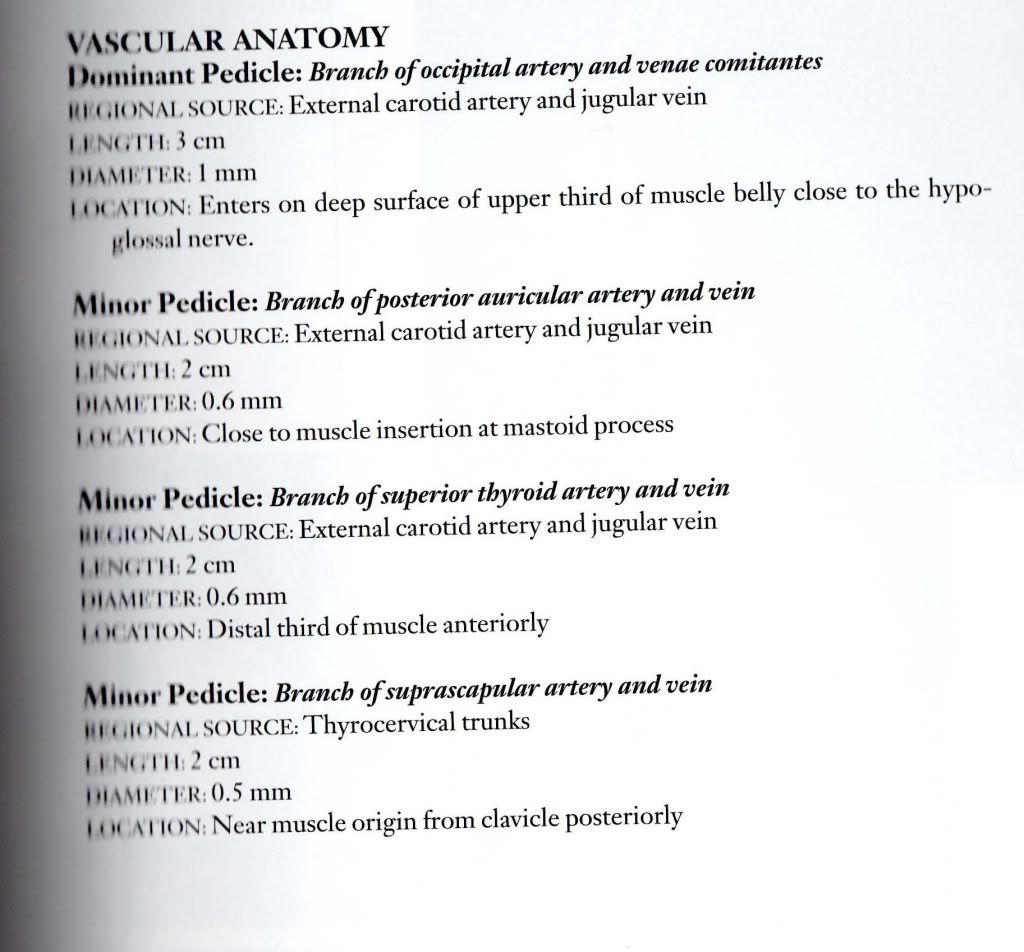
this is the anatomy and the vessels of the sternocleidomastoid muscle (only the arteries here, the veins were of no importance until recently)
http://i1129.photobucket.com/albums/m51 ... oid2-7.jpg
almost 90% of this pair of muscles has venous outflow through the jugulars
Maybe the spasm was some symptom of venous congestion of the muscles.
I am relieved of the neck pain and i can turn and flex my head so easily now.
I hope that this will last forever and so will all my other improvements.
Maybe other people have experienced the same thing.
Muscles have veins, too!
Thank you again Dr Sclafani (and this one is a special 6 months post-op thank you)!
-and thank you Cece for the image uploading advice!
MRI showed some mildly prolapsed cervical disk, so i thought i would live with it forever. I was having physiotherapy and i was taking pain killers almost every second day.
Then, 6 months ago (6/10/2011) i had my angioplasty procedure.
One month later i was talking to Dr Sclafani about the great improvements i already had. I mentioned that my neck pain was unexpectedly disappeared. He replied only "Ah, it was the spasm!"
I found what he meant:
http://i1129.photobucket.com/albums/m51 ... stoid1.jpg
{kind=link}
this is the anatomy and the vessels of the sternocleidomastoid muscle (only the arteries here, the veins were of no importance until recently)
http://i1129.photobucket.com/albums/m51 ... oid2-7.jpg
{kind=link}
almost 90% of this pair of muscles has venous outflow through the jugulars
Maybe the spasm was some symptom of venous congestion of the muscles.
I am relieved of the neck pain and i can turn and flex my head so easily now.
I hope that this will last forever and so will all my other improvements.
Maybe other people have experienced the same thing.
Muscles have veins, too!
Thank you again Dr Sclafani (and this one is a special 6 months post-op thank you)!
-and thank you Cece for the image uploading advice!
getafix
-
mo_en
- Family Member
- Posts: 48
- Joined: Thu Dec 09, 2010 3:00 pm
- Location: Patras, Greece
Re: DrSclafani answers some questions
May i add (ask) that muscles of the neck and upper back with reduced flexibility due to venous outflow obstructions put more strain on neck veins and thus worsen the outflow problem itself (?).