DrSclafani answers some questions
Re: DrSclafani answers some questions
Yes, it was this last time and as far as I know it was ok. My Doc.proposed a 2nd stent (inside the other one) to my right IJV and I said no.

Re: DrSclafani answers some questions
I thank you very much for explaining that to me, this will help me answer this difficult when I am asked it.
Re: DrSclafani answers some questions
So, in a list, the 1% who deteriorate might have:
1) an ongoing exacerbation that began before the venoplasty procedure
2) been negatively affected by the medications and anticoagulants
3) have an exacerbation caused by the procedure, if extreme reflux occurs when the ballooning cuts off flow (would this be only in the 'red face' cases, where the other jugular is fully blocked, or could it occur even if the other jugular is functional?)
4) stopped their DMD post-procedure, flush with optimism, and suffered a relapse
5) been similar to those who never got any improvements, and then the course of MS would lead to deterioration, unrelated to the procedure
I would suggest adding that there is also the possibility of deteriorating if there are complications, such as thrombus. Even with optimized techniques, there can still be a rupture of a balloon in the jugular that damages the vein or other such misfortune.
And the patients who ask msfire about deterioration might not be going to a proceduralist who uses ivus, for example, which has been shown in that abstract to reduce vein injury:
http://www.ccsvicare.org/outreach_update03.html
A really good abstract.
mtf, do you know why he wanted to place an in-stent stent? What is going on inside that stent?
1) an ongoing exacerbation that began before the venoplasty procedure
2) been negatively affected by the medications and anticoagulants
3) have an exacerbation caused by the procedure, if extreme reflux occurs when the ballooning cuts off flow (would this be only in the 'red face' cases, where the other jugular is fully blocked, or could it occur even if the other jugular is functional?)
4) stopped their DMD post-procedure, flush with optimism, and suffered a relapse
5) been similar to those who never got any improvements, and then the course of MS would lead to deterioration, unrelated to the procedure
I would suggest adding that there is also the possibility of deteriorating if there are complications, such as thrombus. Even with optimized techniques, there can still be a rupture of a balloon in the jugular that damages the vein or other such misfortune.
And the patients who ask msfire about deterioration might not be going to a proceduralist who uses ivus, for example, which has been shown in that abstract to reduce vein injury:
http://www.ccsvicare.org/outreach_update03.html
A really good abstract.
mtf, do you know why he wanted to place an in-stent stent? What is going on inside that stent?
Re: DrSclafani answers some questions
Thank you Cece for putting it in a "Coles Notes" version for us non-medics.
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Sounds like a good idea. just do proper things to maintain health of remaining veins,good diet, antiplatelets, anticoagulationmtf wrote:Thanks Dr. S. for your advice.
My left iliac vein was stented too last year and is flowing well. Really don't know what to do now, but I think I have to wait and see what to do.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
correct. occlusion of a vein will make you worse in the short term unless your vein was already >90% stenosed.Cece wrote:So, in a list, the 1% who deteriorate might have:
1) an ongoing exacerbation that began before the venoplasty procedure
2) been negatively affected by the medications and anticoagulants
3) have an exacerbation caused by the procedure, if extreme reflux occurs when the ballooning cuts off flow (would this be only in the 'red face' cases, where the other jugular is fully blocked, or could it occur even if the other jugular is functional?)
4) stopped their DMD post-procedure, flush with optimism, and suffered a relapse
5) been similar to those who never got any improvements, and then the course of MS would lead to deterioration, unrelated to the procedure
I would suggest adding that there is also the possibility of deteriorating if there are complications, such as thrombus. Even with optimized techniques, there can still be a rupture of a balloon in the jugular that damages the vein or other such misfortune.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re:
*bumping an old post for a question*astro wrote:Hi, Dr. Sclafani,
First, I want to echo everyone’s appreciation for your work. Thank you for what you are doing!
I underwent a venogram and angio of my left and right IJV six weeks ago, and thought I’d share what I think are interesting results and ask a few questions.
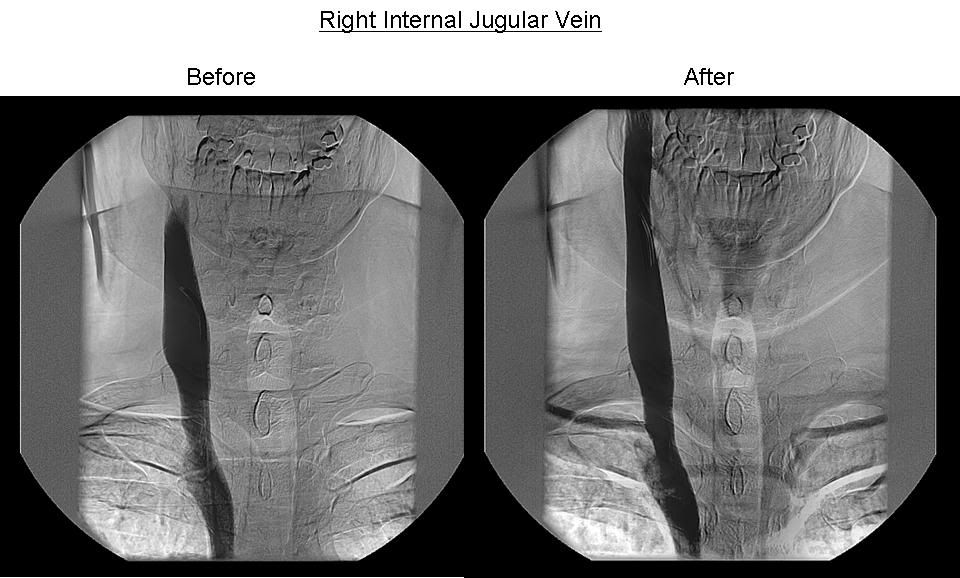
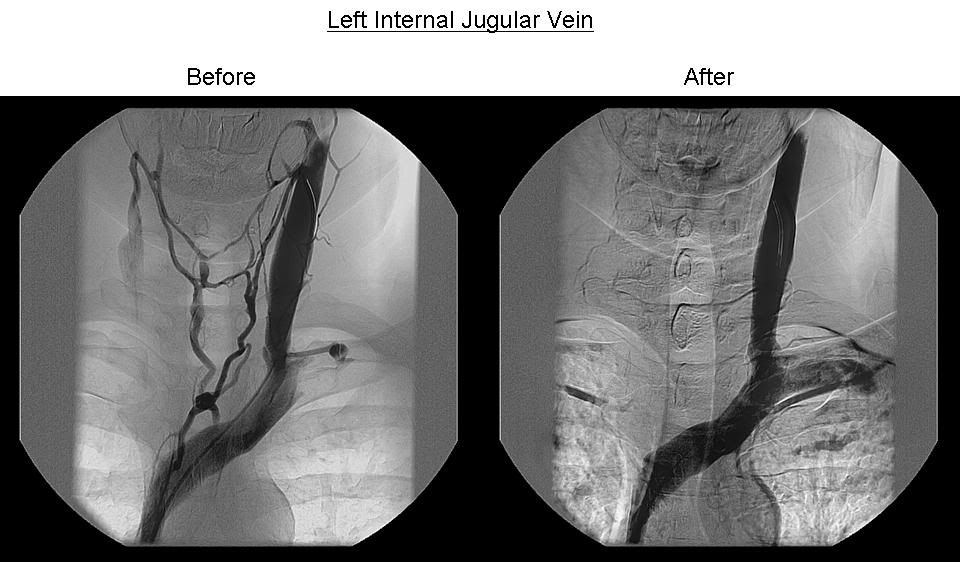
My venogram was performed based on an ultrasound that indicated reflux of 1.3 seconds in my right IJV, but normal flow in my left. During the procedure, we were all very surprised when my venogram showed moderate blockage in my right (consistent with the ultrasound), but more severe blockage and an extensive network of collaterals in the left (contradicting the ultrasound).
The blockage on both sides was low, near my clavicle. If I could show you the animation, you could also see the reflux above my clavicle, including in the left IJV that had gone undetected. My right IJV was then ballooned and flow became normal. My left side blockage was ballooned in two places, and afterward the collaterals immediately disappeared.
However, a “secondary reflux” then appeared lower down, with dye shooting back up into my subclavian vein. You can see this in the “left after” picture. Strange, huh?
Since my procedure, I experienced a brief period of improvement of both cognitive and physical symptoms, but now only the cognitive improvements remain. My legs are in a decline. I am now trying to figure out why, and I hope you might be able to comment:
First, the venogram report indicated that my azygos appeared okay, but the images I have are much less conclusive (in my opinion) than the IJV images. So given your previous posting, I am suspicious that something may have been missed. Do you think it is more likely the azygos blockage was missed, or that my IJV restenosed?
Second, the “secondary reflux” which developed into the subclavian vein makes me wonder what is happening there. Since I still have reflux, do I still have blockage further down? Is this perhaps due to a valve issue? Does the subclavian relate directly to the azygos?
I feel very fortunate that I had the treatment, but my sense is that I still have an issue -- one which many of us might share -- that needs to be addressed.
Re:
Here was your original response back in May 2010. Images are in the post above. I have heard recently from astro (hi astro) and after seeing his images, I was wondering about that reflux into the subclavian. If you saw this in a patient of yours, would you investigate the subclavian for a stenosis there? I'm remembering the patient who had a port in the subclavian, I think it was.drsclafani wrote:Nice images.astro wrote:Hi, Dr. Sclafani,
First, the venogram report indicated that my azygos appeared okay, but the images I have are much less conclusive (in my opinion) than the IJV images. So given your previous posting, I am suspicious that something may have been missed. Do you think it is more likely the azygos blockage was missed, or that my IJV restenosed?
Second, the “secondary reflux” which developed into the subclavian vein makes me wonder what is happening there. Since I still have reflux, do I still have blockage further down? Is this perhaps due to a valve issue? Does the subclavian relate directly to the azygos?
I feel very fortunate that I had the treatment, but my sense is that I still have an issue -- one which many of us might share -- that needs to be addressed.
First, the narrowings are not high grade compared to many others i have seen. What is your EDSS?
I see a clear cut stuck valve on the left side. They are pesky sometimes, need cutting balloons and possibly will ultimately need stents. The reflux in the subclavian is physiological, depending upon the cardiac output, and the volume of contrast injected. The subclavian veins should not have valves there so reflux is not surprising and is seen often during these studies.
Zamboni says he is often seeing an abnormal asygous
Some of these pathologies are quite subtle
I find IVUS very helpful
Re: DrSclafani answers some questions
Dear Dr. S,
I’m SPMS for a long time and I’m wheelchair bonded. I think that I’m worse faster after the stent in my left IG. Meaning the fatigue is overwhelming and I have cardiac arrithms (the Doc. said they are benign since after tests I’ve done to my heart and it’s fine). So, when I say I have to wait and see I mean I don’t know what to do right now and with whom. Btw, I'm taking antiplatelets (plavix and aspirin) and not anticoagulation med .
Cece
The stent in my right jugular is not ok also, moved a bit down and keeps closing (??)
I’m SPMS for a long time and I’m wheelchair bonded. I think that I’m worse faster after the stent in my left IG. Meaning the fatigue is overwhelming and I have cardiac arrithms (the Doc. said they are benign since after tests I’ve done to my heart and it’s fine). So, when I say I have to wait and see I mean I don’t know what to do right now and with whom. Btw, I'm taking antiplatelets (plavix and aspirin) and not anticoagulation med .
Cece
The stent in my right jugular is not ok also, moved a bit down and keeps closing (??)
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: Re:
AStroCece wrote:*bumping an old post for a question*astro wrote:Hi, Dr. Sclafani,
First, I want to echo everyone’s appreciation for your work. Thank you for what you are doing!
I underwent a venogram and angio of my left and right IJV six weeks ago, and thought I’d share what I think are interesting results and ask a few questions.
My venogram was performed based on an ultrasound that indicated reflux of 1.3 seconds in my right IJV, but normal flow in my left. During the procedure, we were all very surprised when my venogram showed moderate blockage in my right (consistent with the ultrasound), but more severe blockage and an extensive network of collaterals in the left (contradicting the ultrasound).
The blockage on both sides was low, near my clavicle. If I could show you the animation, you could also see the reflux above my clavicle, including in the left IJV that had gone undetected. My right IJV was then ballooned and flow became normal. My left side blockage was ballooned in two places, and afterward the collaterals immediately disappeared.
However, a “secondary reflux” then appeared lower down, with dye shooting back up into my subclavian vein. You can see this in the “left after” picture. Strange, huh?
Since my procedure, I experienced a brief period of improvement of both cognitive and physical symptoms, but now only the cognitive improvements remain. My legs are in a decline. I am now trying to figure out why, and I hope you might be able to comment:
First, the venogram report indicated that my azygos appeared okay, but the images I have are much less conclusive (in my opinion) than the IJV images. So given your previous posting, I am suspicious that something may have been missed. Do you think it is more likely the azygos blockage was missed, or that my IJV restenosed?
Second, the “secondary reflux” which developed into the subclavian vein makes me wonder what is happening there. Since I still have reflux, do I still have blockage further down? Is this perhaps due to a valve issue? Does the subclavian relate directly to the azygos?
I feel very fortunate that I had the treatment, but my sense is that I still have an issue -- one which many of us might share -- that needs to be addressed.
it is not surprising that the ultrasound underestimated the problems. I always look at that test as a simple red light greenlight. two criteria positive, justification for an invasive procedure. One criterial positive -reevaluate based on clinical scenario. No criteria positive, think of another cause of demyelinization.
It is however surprising in this case where a thickened immobile left valve is quite evident on the venogram. That could have been seen on Doppler.
Now on to treatment...very short improvement in motor function, improved cognition. Why so short? Probably underdilatation is my guess without knowing you or your symptoms.
do you know what size balloons and what pressure were used?
I have found that IVUS is invaluable for diagnosis of lesions in the aygous vein. In my randomized review of 30 Azygous lesions, venography missed 20% of the mostly valvular stenoses
I gave up one of my treatment sites because I didnt have IVUS there. I guess that indicates my feelings on this issue.
By the way, i dont see any difference in the two right venograms, do you?
With regard to the reflux into the subclavian vein, i really cant make a comment
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: Re:
Wow, may 2010. My current answer is consistent but clearer now. Certainly NO cutting balloons or stents are necessary for such problems, certainly without another more realistic treatment.Cece wrote:Here was your original response back in May 2010. Images are in the post above. I have heard recently from astro (hi astro) and after seeing his images, I was wondering about that reflux into the subclavian. If you saw this in a patient of yours, would you investigate the subclavian for a stenosis there? I'm remembering the patient who had a port in the subclavian, I think it was.drsclafani wrote:Nice images.astro wrote:Hi, Dr. Sclafani,
First, the venogram report indicated that my azygos appeared okay, but the images I have are much less conclusive (in my opinion) than the IJV images. So given your previous posting, I am suspicious that something may have been missed. Do you think it is more likely the azygos blockage was missed, or that my IJV restenosed?
Second, the “secondary reflux” which developed into the subclavian vein makes me wonder what is happening there. Since I still have reflux, do I still have blockage further down? Is this perhaps due to a valve issue? Does the subclavian relate directly to the azygos?
I feel very fortunate that I had the treatment, but my sense is that I still have an issue -- one which many of us might share -- that needs to be addressed.
First, the narrowings are not high grade compared to many others i have seen. What is your EDSS?
I see a clear cut stuck valve on the left side. They are pesky sometimes, need cutting balloons and possibly will ultimately need stents. The reflux in the subclavian is physiological, depending upon the cardiac output, and the volume of contrast injected. The subclavian veins should not have valves there so reflux is not surprising and is seen often during these studies.
Zamboni says he is often seeing an abnormal asygous
Some of these pathologies are quite subtle
I find IVUS very helpful
I am less impressed with the treatment of the right IJV than i might have been back in 2010. How is Astro? Was another treatment attempted? Shame. my guess is too small a balloon was used , but that is better, i suppose, than too large!
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
smells like intimal hyperplasia and that is why another stent was suggested. (my guess)mtf wrote:Dear Dr. S,
I’m SPMS for a long time and I’m wheelchair bonded. I think that I’m worse faster after the stent in my left IG. Meaning the fatigue is overwhelming and I have cardiac arrithms (the Doc. said they are benign since after tests I’ve done to my heart and it’s fine). So, when I say I have to wait and see I mean I don’t know what to do right now and with whom. Btw, I'm taking antiplatelets (plavix and aspirin) and not anticoagulation med .
Cece
The stent in my right jugular is not ok also, moved a bit down and keeps closing (??)
mtf, it is difficult for me to gie clear advice, not knowning the extent of your treatment and the current state of all the eins.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: Re:
Cece wrote:Here was your original response back in May 2010. Images are in the post above. I have heard recently from astro (hi astro) and after seeing his images, I was wondering about that reflux into the subclavian. If you saw this in a patient of yours, would you investigate the subclavian for a stenosis there? I'm remembering the patient who had a port in the subclavian, I think it was.drsclafani wrote:Nice images.astro wrote:Hi, Dr. Sclafani,
First, the venogram report indicated that my azygos appeared okay, but the images I have are much less conclusive (in my opinion) than the IJV images. So given your previous posting, I am suspicious that something may have been missed. Do you think it is more likely the azygos blockage was missed, or that my IJV restenosed?
Second, the “secondary reflux” which developed into the subclavian vein makes me wonder what is happening there. Since I still have reflux, do I still have blockage further down? Is this perhaps due to a valve issue? Does the subclavian relate directly to the azygos?
I feel very fortunate that I had the treatment, but my sense is that I still have an issue -- one which many of us might share -- that needs to be addressed.
First, the narrowings are not high grade compared to many others i have seen. What is your EDSS?
I see a clear cut stuck valve on the left side. They are pesky sometimes, need cutting balloons and possibly will ultimately need stents. The reflux in the subclavian is physiological, depending upon the cardiac output, and the volume of contrast injected. The subclavian veins should not have valves there so reflux is not surprising and is seen often during these studies.
Zamboni says he is often seeing an abnormal asygous
Some of these pathologies are quite subtle
I find IVUS very helpful
Wow, may 2010. My current answer is consistent but clearer now. Certainly NO cutting balloons or stents are necessary for such problems, certainly without another more realistic treatment.
I am less impressed with the treatment of the right IJV than i might have been back in 2010. How is Astro? Was another treatment attempted? Shame. my guess is too small a balloon was used , but that is better, i suppose, than too large!
talking about the interpretation of the images in 2010 led me to remember that I knew i was treating valves way back in early 2010. I just recently saw my third patient from two full years ago, doing so well. in my report in January 2010 I diagnosed valvular stenosis on IVUS.So that sets the record straight, i think
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Hi all, I'm putting this out there as a prompt for people in the know.
Has anyone experimented with cerebral oximeters before and after PTA and also as a follow up tool.
My reading on this and input from others I have contacted from a broad spectrum of professionals is that if it is used appropriately it will become a supportive tool in the treatment process and likely a tool in the dx of CCSVI as well once there is familiarity with the technique and understanding of the implications!
Stenosis equals low oxygen levels so measuring the levels MUST be a tool to indicate the vast array of issues that are 'caused' down stream, be that CCSVI symptoms or other issues that are beginning to be understood about slow flows and refluxing.
I welcome comments on this to get some research going, soon!
Regards Nigel
Has anyone experimented with cerebral oximeters before and after PTA and also as a follow up tool.
My reading on this and input from others I have contacted from a broad spectrum of professionals is that if it is used appropriately it will become a supportive tool in the treatment process and likely a tool in the dx of CCSVI as well once there is familiarity with the technique and understanding of the implications!
Stenosis equals low oxygen levels so measuring the levels MUST be a tool to indicate the vast array of issues that are 'caused' down stream, be that CCSVI symptoms or other issues that are beginning to be understood about slow flows and refluxing.
I welcome comments on this to get some research going, soon!
Regards Nigel
Re: DrSclafani answers some questions
Nigel, here is a somewhat relevant q&a from way back. I suggested intravascular jugular bulb venous oxygen saturation monitoring with a catheter, Dr. Sclafani answered:
http://www.thisisms.com/forum/chronic-c ... ml#p110957
http://www.thisisms.com/forum/chronic-c ... ml#p110957
The only thing that comes close to what you're suggesting that I know has been done is Dr. Hubbard's before- and after- angio fMRIs with BOLD.drsclafani wrote:venous oxygenation represents the residual oxygen after metabolism
this could be because the arterial oxygenation starts low, or the flow state is slow and more oxygen can be extracted, or the brain metabolism is greater and requires more oxygen
There are other techniques to measure cerebral blood flow that might be more valuable. putting probes in jugular veins might be a potential cause of narrowing
http://en.wikipedia.org/wiki/Functional ... ce_imagingThe procedure [fMRI] is similar to MRI but uses the change in magnetization between oxygen-rich and oxygen-poor blood as its basic measure.