Hi Dr. Sclafani,
I have a new symptom in my left leg, could this mean a new stenosis, or perhaps a restenosis?
My left side is my strong side, so this concerns me. (Last procedure, mid June)
Thank you
DrSclafani answers some questions
-
dlynn

- Family Elder
- Posts: 229
- Joined: Thu Jul 28, 2011 2:00 pm
-
NZer1
- Family Elder
- Posts: 1624
- Joined: Thu Feb 18, 2010 3:00 pm
- Location: Rotorua New Zealand
Re: DrSclafani answers some questions
From CCSVI in New Zealand:https://www.facebook.com/pages/CCSVI-in ... 984?ref=ts
"Sal Sclafani, MD
Interested in CCSVI Treatment? Check out my new website!"
http://www.ccsvicare.org/
CCSVI Care | Salvatore Sclafani, MD
www.ccsvicare.org
CCSVI Care, Liberation by Salvatore JA Sclafani, MD
"Sal Sclafani, MD
Interested in CCSVI Treatment? Check out my new website!"
http://www.ccsvicare.org/
CCSVI Care | Salvatore Sclafani, MD
www.ccsvicare.org
CCSVI Care, Liberation by Salvatore JA Sclafani, MD
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
For those who watched Dr. Sclafani on the expo, or those who didn't, were any of these topics of interest?
1 - If a patient has a physiological stenosis due to muscle compression of the jugular, rather than placing a stent inside the vein, Dr. Sclafani suggested a pharmacological solution to the muscle. I am imagining botox but it is the only muscle paralyzer that I know. Would paralyzing the muscle be what is needed, or would it be a muscle relaxant?
2 - He's seen the sort of comradery we show each other in one other group: the NYPD. Quite a compliment.
3 - There is more blood going through your kidney than through your brain. Ok, we've discussed this one before. Still a surprising quantity of flow.
4 - When our neurons are not dead but merely dysfunctional, the restoration of blood flow leading to improvements is the only way to explain those improvements. It can't be anything but related to vascular draining.
5 - He was asked what might predispose someone toward clotting. Answer was: a hypercoaguability disorder, smoking, being on birth control pills, going to an IR who doesn't believe in anticoagulation.
6 - This was interesting, it's a continuation of the clotting question. Why would a vein thrombose? Overdilatation. Aggressive treatment of hypoplasia. If it's the left jugular vein. If the vein has a very large collateral, such as if flow is diverting through another vein, then there is less flow through the jugular, and that reduction in flow increases chances of clotting. If there's a stenosis in the sigmoid sinus, the same problem occurs, where there is less flow in the jugular and the reduced flow means greater chance of clotting.
7- Valve is immobile because it's not elastic. The rest of the vein can distend and collapse, but not the valve. Recurrent valvular stenosis is very different than scarring of the vein.
8- He saw his mother recently, and his mother asked him, "Why do you work so hard?" His answer was a good one....
1 - If a patient has a physiological stenosis due to muscle compression of the jugular, rather than placing a stent inside the vein, Dr. Sclafani suggested a pharmacological solution to the muscle. I am imagining botox but it is the only muscle paralyzer that I know. Would paralyzing the muscle be what is needed, or would it be a muscle relaxant?
2 - He's seen the sort of comradery we show each other in one other group: the NYPD. Quite a compliment.
3 - There is more blood going through your kidney than through your brain. Ok, we've discussed this one before. Still a surprising quantity of flow.
4 - When our neurons are not dead but merely dysfunctional, the restoration of blood flow leading to improvements is the only way to explain those improvements. It can't be anything but related to vascular draining.
5 - He was asked what might predispose someone toward clotting. Answer was: a hypercoaguability disorder, smoking, being on birth control pills, going to an IR who doesn't believe in anticoagulation.
6 - This was interesting, it's a continuation of the clotting question. Why would a vein thrombose? Overdilatation. Aggressive treatment of hypoplasia. If it's the left jugular vein. If the vein has a very large collateral, such as if flow is diverting through another vein, then there is less flow through the jugular, and that reduction in flow increases chances of clotting. If there's a stenosis in the sigmoid sinus, the same problem occurs, where there is less flow in the jugular and the reduced flow means greater chance of clotting.
7- Valve is immobile because it's not elastic. The rest of the vein can distend and collapse, but not the valve. Recurrent valvular stenosis is very different than scarring of the vein.
8- He saw his mother recently, and his mother asked him, "Why do you work so hard?" His answer was a good one....
-
NZer1
- Family Elder
- Posts: 1624
- Joined: Thu Feb 18, 2010 3:00 pm
- Location: Rotorua New Zealand
Re: DrSclafani answers some questions
Haven't listened to the Conference yet and appreciate you notes Cece.
Interesting how collateral's are a problem in some cases, they may need to be targeted to close. If clotting etc is a problem in dilating veins with valve problems, maybe a cross over treatment could happen. The problem becomes the cure, so to say!
N
Interesting how collateral's are a problem in some cases, they may need to be targeted to close. If clotting etc is a problem in dilating veins with valve problems, maybe a cross over treatment could happen. The problem becomes the cure, so to say!
N
-
DougL

- Family Elder
- Posts: 384
- Joined: Mon Jul 11, 2011 2:00 pm
Re: DrSclafani answers some questions
Dr. S - i see the posts on Facebook. great looking website.
any update on moving to Manhattan?
any update on moving to Manhattan?
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
Wow, didn't think of that. But if it's a big collateral, I can't see wanting to close it off and have less outflow, especially since there's no guarantee the jugular itself will stay open.Interesting how collateral's are a problem in some cases, they may need to be targeted to close.
Yesterday he said that 80-85% of the stenoses he saw were valve problems. So this would be the majority of us. He's also said that clotting has not been a problem with his new treatment protocols (sizing balloons with ivus, using pradaxa and aspirin) and he's had only 2 thromboses in patients who discontinued the anticoagulation early.If clotting etc is a problem in dilating veins with valve problems, maybe a cross over treatment could happen. The problem becomes the cure, so to say!
N
But the question is what can be done about a vein with an inflow problem, such as a large collateral, that by reducing flow through the jugular ends up increasing the risk of clotting? Proper anticoagulation? Don't sit up? Maybe such a patient should be done at a hospital, not an outpatient clinic, because they need to lie flat for longer after the procedure (since much more flow goes through the jugulars when lying flat) and could be kept overnight.
-
Donnchadh

- Family Elder
- Posts: 526
- Joined: Sat Jan 23, 2010 3:00 pm
Re: DrSclafani answers some questions
Dr. Sclafani:
Has anyone been able to treat stenois in the sigmoid sinus yet?
Donnchadh
Has anyone been able to treat stenois in the sigmoid sinus yet?
Donnchadh
Kitty says, "Take that, you stenosis!"
Got MS?.....Get Liberated!
Got MS?.....Get Liberated!
-
Cece
- Family Elder
- Posts: 9335
- Joined: Mon Jan 04, 2010 3:00 pm
- Contact:
Re: DrSclafani answers some questions
Here's a past case study that shows the only treatment I know of that Dr. Sclafani has done in a patient's left signoid sinus. He flushed out an old clot:
http://www.thisisms.com/forum/chronic-c ... ml#p166815
This wouldn't help if it's a malformed sinus or if it's recanalized from some prior clotting, only if it happens to be an old clot that responds to flushing.
Your question still stands, because we don't know if Dr. Zamboni or one of the other IRs or a neurointerventional radiologist has gotten anywhere with this.
http://www.thisisms.com/forum/chronic-c ... ml#p166815
This wouldn't help if it's a malformed sinus or if it's recanalized from some prior clotting, only if it happens to be an old clot that responds to flushing.
Your question still stands, because we don't know if Dr. Zamboni or one of the other IRs or a neurointerventional radiologist has gotten anywhere with this.
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I already answered this on the IJ trauma thread but here it is again:Donnchadh wrote:Dr. Sclafani:
Has anyone been able to treat stenois in the sigmoid sinus yet?
Donnchadh
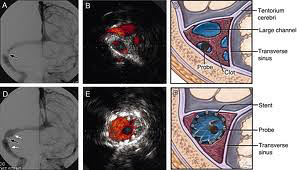
stenoses of the dural sinus has been treated by stenting. this has been published. Images in top row are before stenting. arrows in two leftside images point to the stenosis. The article was speaking about the treatment of the stenosis but the use of IVUS for to monitor the treatment of these stenoses.Donnchadh wrote:Personally I am convinced that my problems are entirely due to a severe ladder accident I had back in 1990. The day before the accident, I was in great shape with absolutely no neurological problems of any kind. From the day of the accident forward, my neurological problems progressively became worse. I have had three separate procedures done, by three different Interventional radiologists, and they were able to identify and correct some of the damage.
What is left is stenosis in the sigmoid sinus, and no one knows how to treat it yet. I have evolved my own DIY iron removal procedure, which is keeping me stable. Without the three procedures (which could be done by one procedure today based on improvements) and the iron removal, I would be in very bad shape.
Donnchadh
DrS
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
The stented renal vein also requires followup but because stenosis or occlusion are not common, the surveillance is not so urgent. I have not seen any thrombus in a renal stent yet. Renal vein stents seem to stay open longer, with a higher frequency and without stenosis. This is perhaps due to the fact that flow is continuous and very significant with few collaterals to compete.pklittle wrote:DrS,
Questions for you... can you tell us about renal stent followup? Is it the same as jugular stent followup at 3 months? Can the flow be clearly seen on ultrasound? Have you seen any thrombus in a renal stent? How many cases of nutcracker syndrome have you diagnosed and stented?
thanks
Abdominal ultrasound is the primary technique of imaing with analysis of velocities and Bmode abnormalities being the primary observations.
I havent done thef ull analysis yet. probably about ten.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
It is a good question. We see many cases of external jugular and anterior jugular veins as collaterals for the IJV.mo_en wrote:Dear Doctor, two questions:
1. How often have you seen the external jugular vein be used as a collateral of the internal?
2. Provided that the above is true, wouldn't be useful to check and restore a probable valve problem in the external?
I did see one case with a larger external jugular vein whose valve appeared to be abnormal. I did dilate it, but that was because the IJV was hypoplastic and remained with stenoses after venoplasty. In order to get blood flow through the IJV as a collateral, it was necessary to open the immobile valve. I am not sure if that was a good idea but i did it.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
many azygous and IJV stenoses are immobile valves. However hypoplasias, webs, septum and membrane also occur. The lesions of the may thurner syndrome and the nutcracker syndrome are actually compression stenoses, as are some of the upper jugular stenoses at the second cervical vertebraePointsNorth wrote:Dr. S,
Are the stenoses found in vessels other than the IJVs valvular in nature? Is this relevant in any way?
BTW-I read that tarsiers can be kept as pets!
PN
S
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
THEGREEKFROMTHED
- Family Elder
- Posts: 162
- Joined: Sat Mar 27, 2010 3:00 pm
Re: DrSclafani answers some questions
Can you effectively treat a kanootin valve at this juncture in your procedures? Mine is hurtin like a mutha.
yours truly
yours truly
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
wow, we are having surge of great questions. I havent been coming here as often because there have been few questions. Now I come back and there is a boatload of work for me!mo_en wrote:One more: How can one tell whether a vein is hypoplastic or simply narrow due to small blood flow? If the accumulation of lesions in the spinal cord diminished the available room in the vertebral column or exerted pressure on vertebral plexus, could this result in reduced spinal flow capacity and, subsequently, less blood volume in the lumbar veins?
it is usually simple to tell the difference: IVUS.
A unloaded vein shrinks but it can fill so you can see expansion of the vein after certain manuevers.
the hypoplastic vein never developed or enlarged with development. Such veins are fixed in their diameters.
so IVUS wins this battle easily.
The second question about the lumbar veins has a trick answer. Lesion volume compression of the lumbar veins does not occur. During fetal development, the spinal cord stops growing as the spine keeps growing. As such the spinal cord ends about the 12 thoracicvertebrae. The nerve roots of the lumbar spinal cord travel down the spine to exit at the appropriate nerve root. so spinal lesions are not in the lumbar spine. This is not the cause of the hypoplasia of the lumbar veins.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
it is the volume that is the concern. The plumber in me can answer this one:CureOrBust wrote:Is it the rapid flow OR the question of what is causing it that raises our concern?Cece wrote:If rapid flow in the azygous looks identical to flow in the azygous when nutcracker syndrome is present, and nutcracker syndrome may cause chronic fatigue, could my rapid flow in my azygous be causing fatigue?
take a 1 inch drain pipe and put flow through it....it works.
take a 2 inch pipe and put the same volume through it and it moves faster but it doesnt back up
take a 1 inch pipe and put double or triple the volume through it and it just might overflow, leaking along the wall and possibly just staining the flooded area.
take a 1 inch drain and block most of it with leaves, and it will also back up
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com